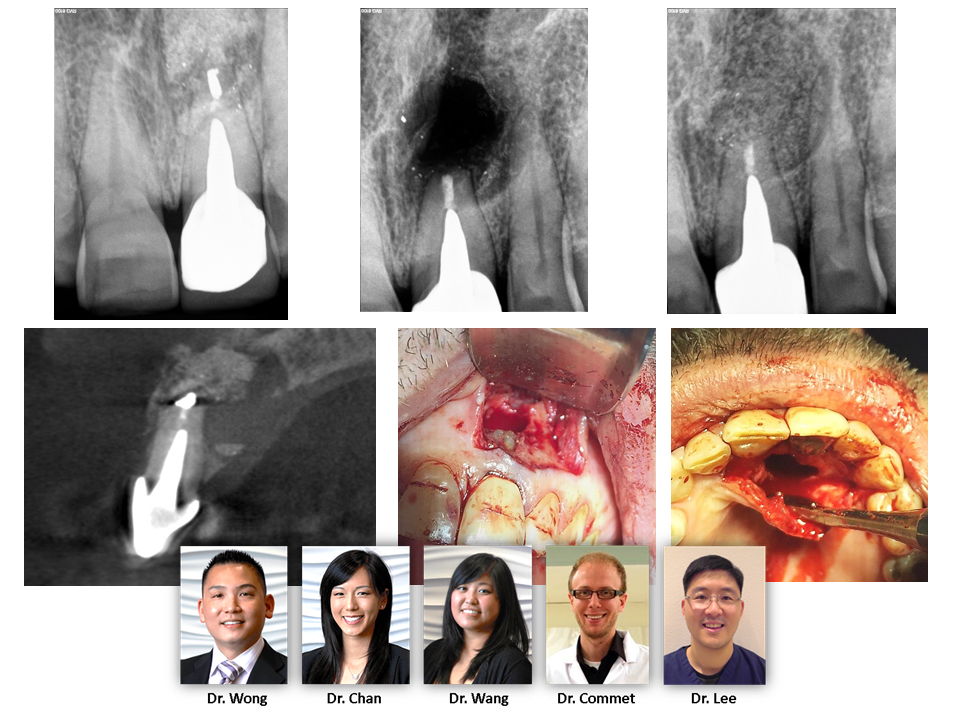
CBCT IMAGING – As many of us are aware, CBCT imaging applications for dentistry are growing at an exponential rate. This case highlights an unusual scenario where the patient received an apicoectomy on tooth #9 ~25 years prior to presentation. His chief complaint was a large sinus tract that had recently developed. Convential PA shows a moderate diameter lucency around the root apex. However, the …CBCT volume highlights an existing osseous graft (later revealed to be bovine bone graft through histology) that is infected and encapsulated by soft tissue. The native bone destruction is actually quite large and perforated on […]
CBCT Imaging