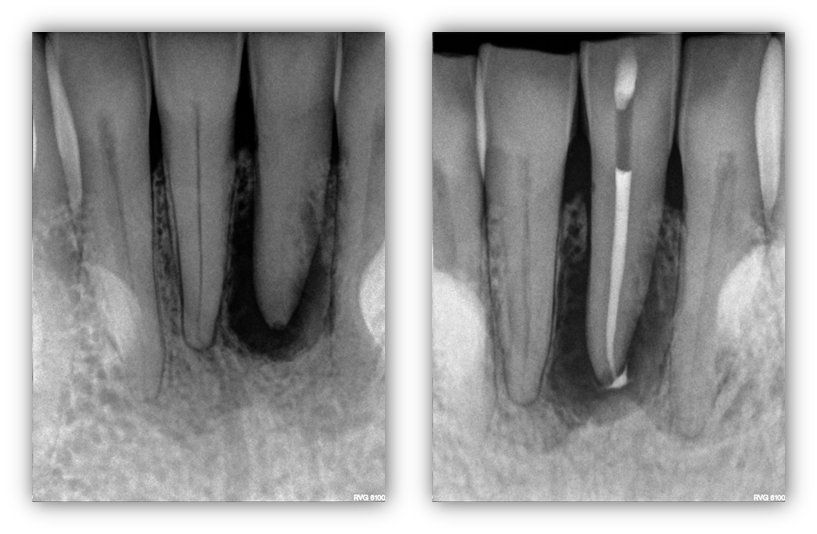
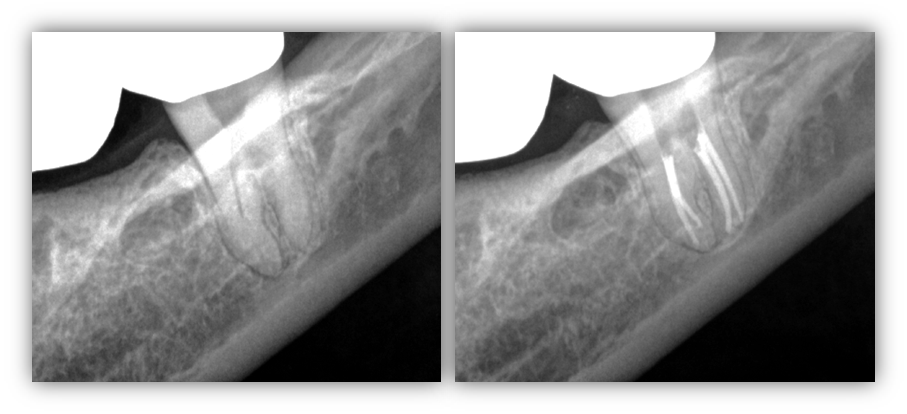
ENDODONTIC SURGERY: Here we present our patient, 33yo health female, who presented with a swelling in the mandibular central area. Root canal treatment when rendered when the patient was an adolescent. Years later, a periapical lesion developed with what appears to be a resorption defect that was not filled at the time of the original fill. We decided to so apicoectomy with conventional root end resection and retrofill, cortical allograft and resorbable membrane. As one can see, the entire buccal surface of the tooth was exposed due to the pathology. Upon post surgical follow-up and secondary recall, the surgical area […]
ENDODONTIC SURGERY…