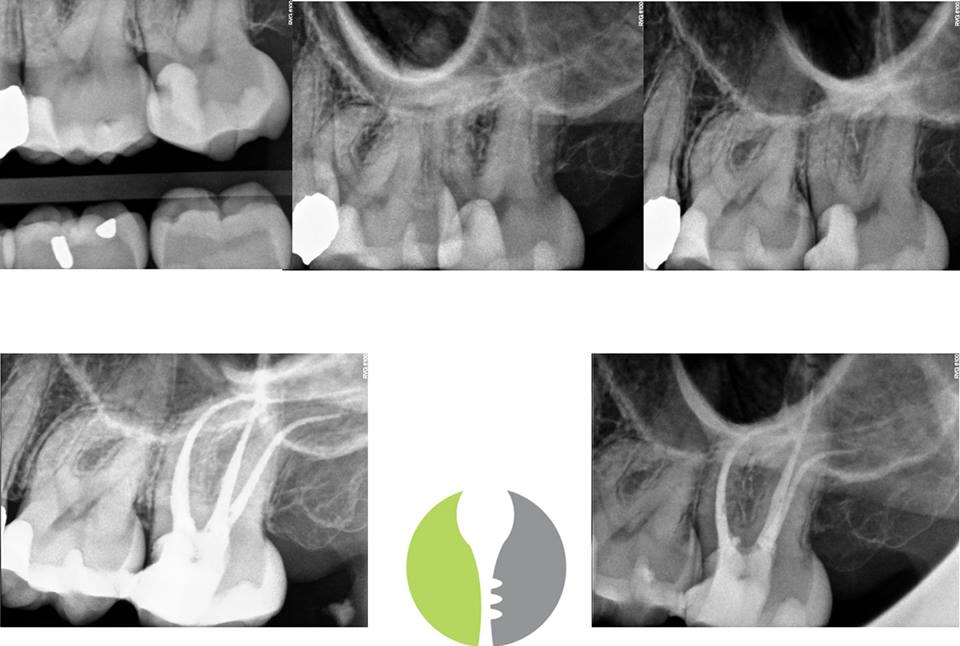
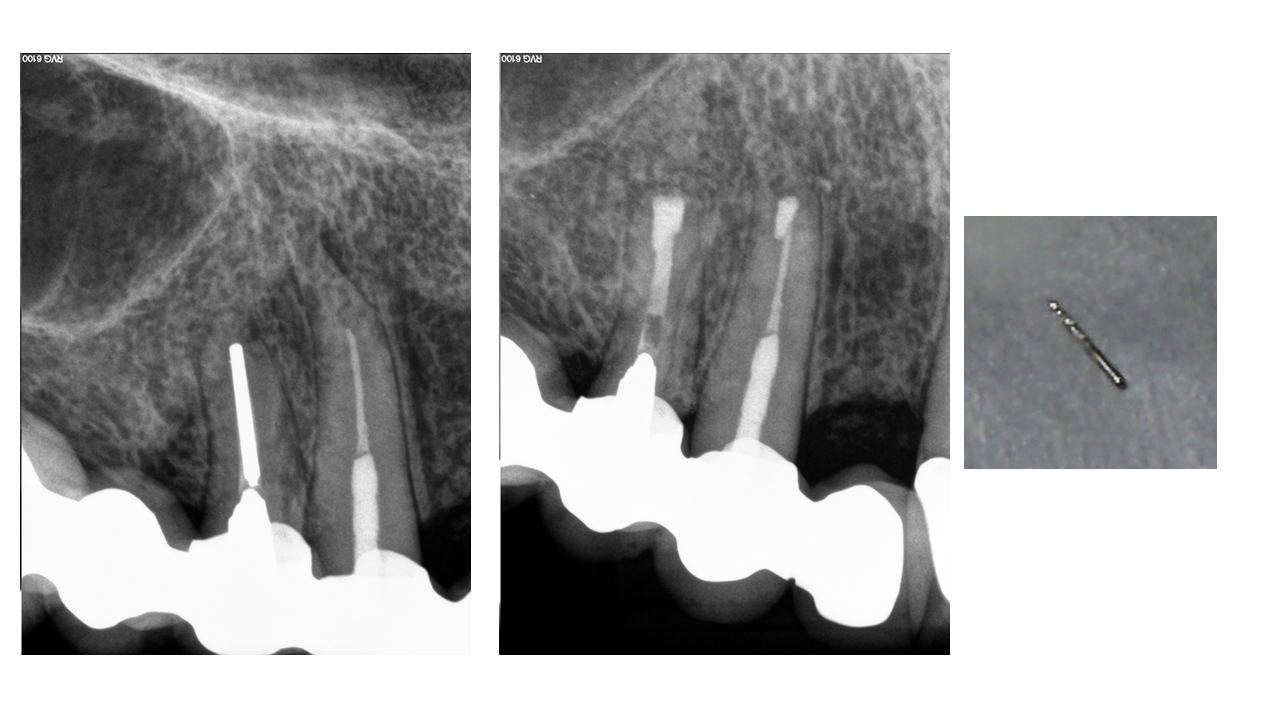
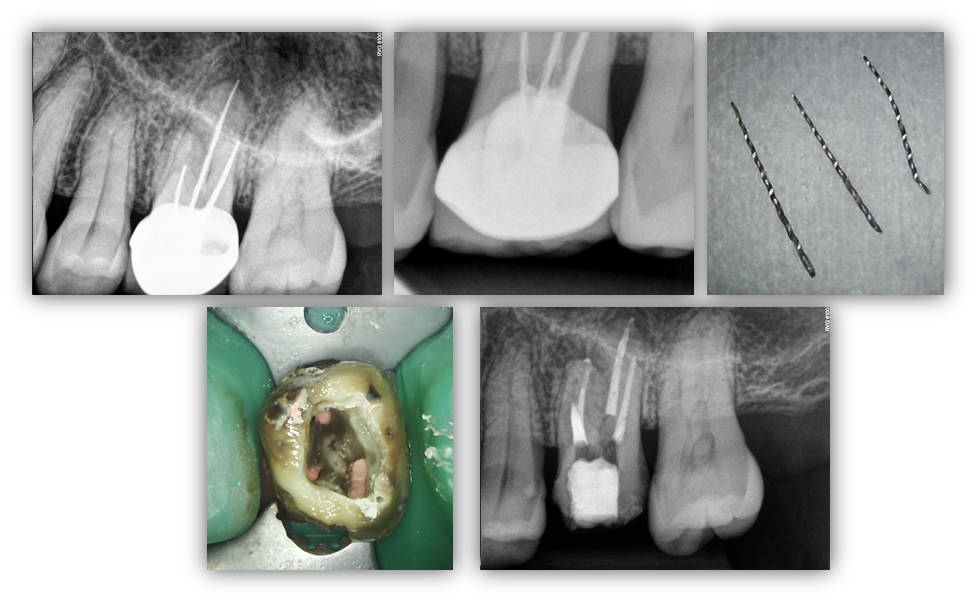
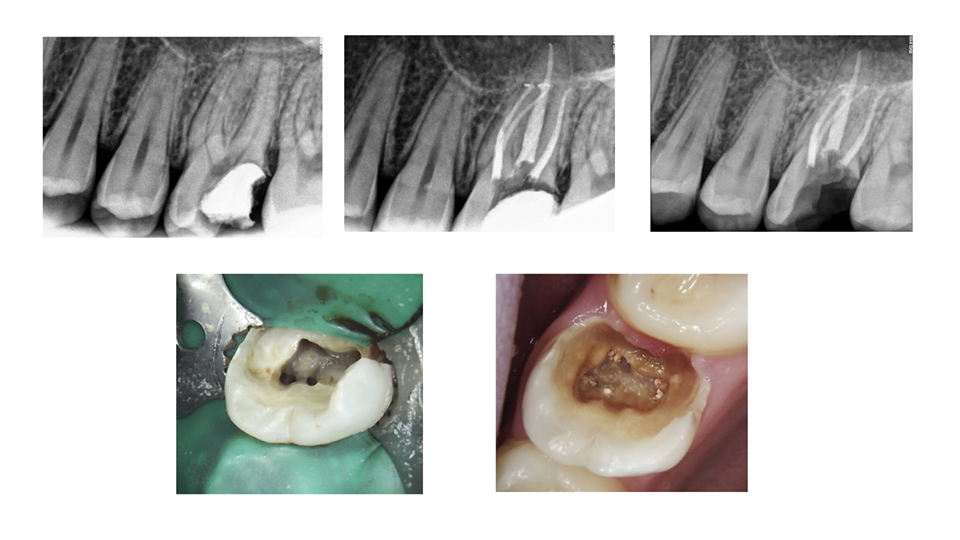
PATIENT MANAGEMENT AND ENDODONTIC TREATMENT: It is not always the anatomy that is difficult in the aspect of treatment. However, added factors can compound case difficulty such as minimal opening, unfavorable angulation towards the cheek, the position of being last tooth in the mouth, AND LONG (WL – 24mm) Curvy Calcified (MB2) Anatomy. At first glance, this just looks like a “run of the mill” root canal with some nice curvatures. However, it is important to note that we treat people, not just teeth. […]
PATIENT MANAGEMENT AND ENDODONTIC TREATMENT