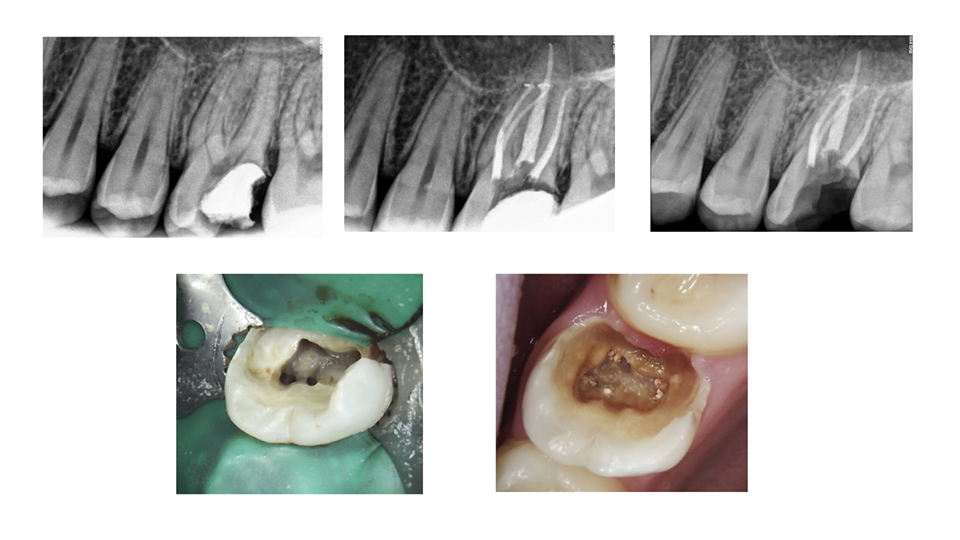
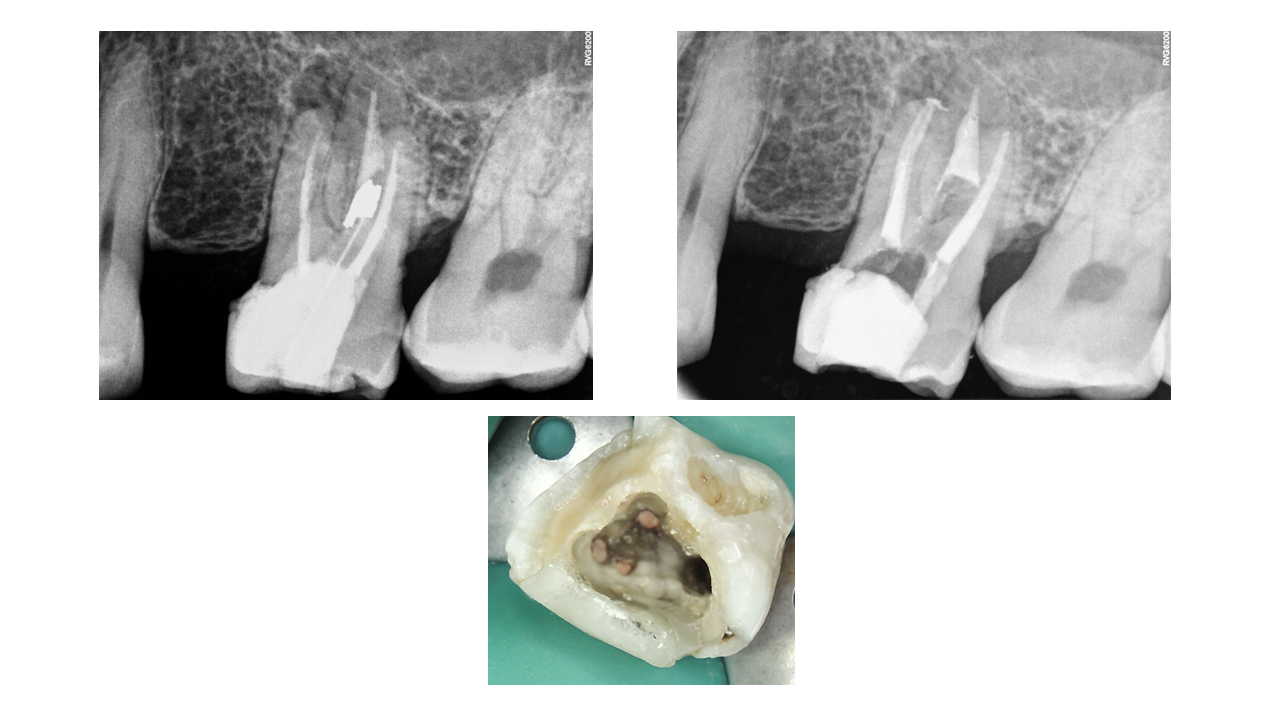
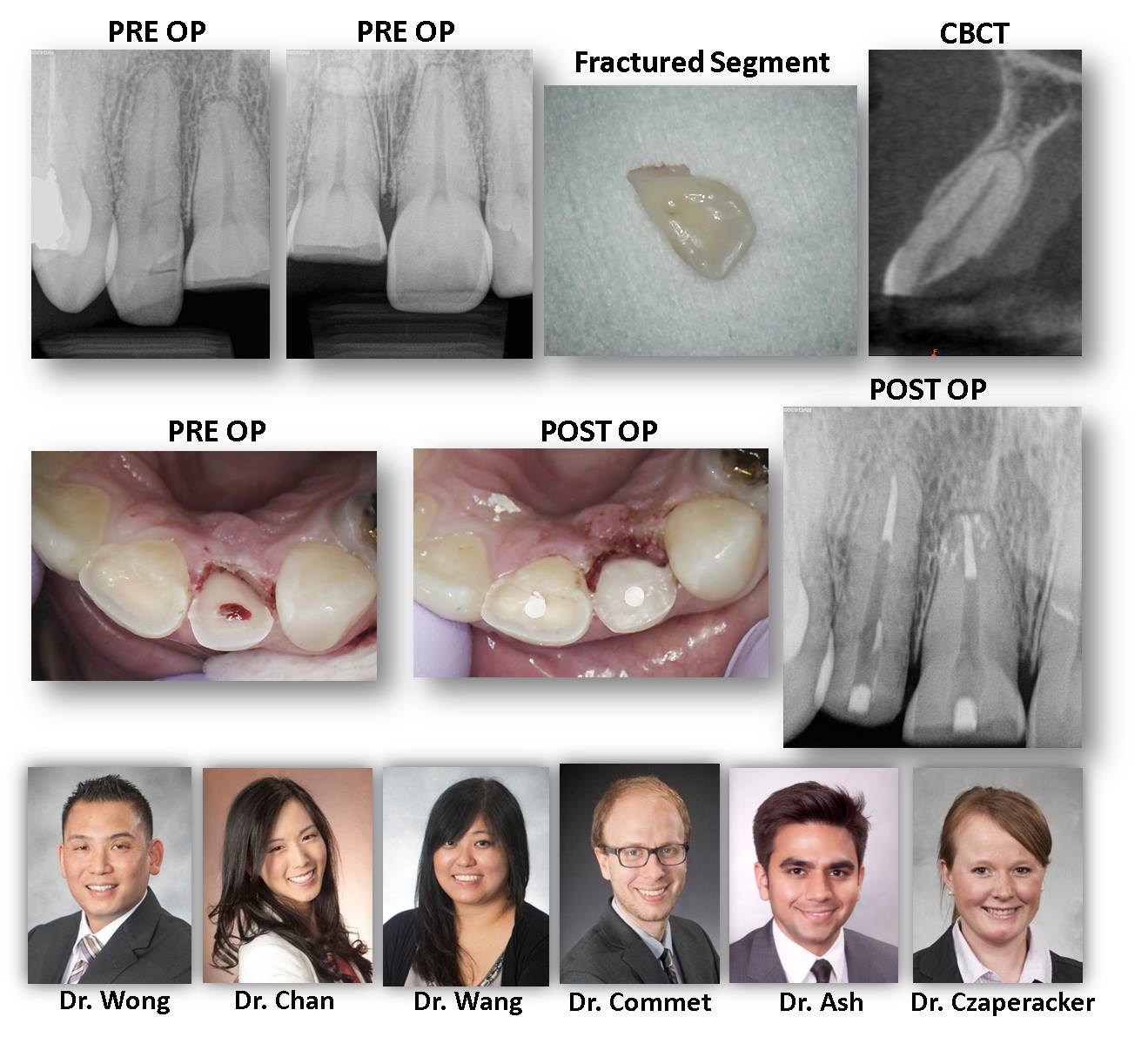
WHY IT IS USEFUL IF YOUR ENDODONTIST CAN DO PERMANENT RESTORATIVE TX: While as endodontists, we always defer core and crown fabrication to the restorative expert (the patients general dentist), we do offer core placement and crown repair for those dentists who request it of us. Here is a great example of why it can be useful to have the core build-up completed at the time of RCT. You will see intra-op photo (5 canal #14) compared with a 6 month recall with gross caries throughout the entire access after the patient failed to have the tooth restored in a […]
ENDODONTISTS AND PERMANENT RESTORATIONS…