IS THIS “REGENERATION”? Here is an interesting case of a 7yo healthy female who had a history of sustained odontogenic trauma from an incident on the playground. At the time of presentation, the patient had buccal swelling of #9, signs of arrested development of the tooth, Grade III mobility and incisal edges of both maxillary centrals with several millimeters of discrepency. Several factors impacted our treatment decision, age being most significant. We decided to disinfect the tooth first and attempt regeneration to see if we couldn’t get the tooth to continue to develop. At 1 year post treatment the patient […]
Category: Endodontic Treatment
IS THIS "REGENERATION"?
HOPELESS PROGNOSIS?
HOPELESS PROGNOSIS?
HOPELESS PROGNOSIS?: Based on the pre-operative PA, many dentists would suggest to their patients that this tooth has a poor or hopeless prognosis. Clinically it had a 12 mm probing to the apex and radiographically it has a large apical lesion that was confirmed to extend around the entire MB root on CBCT. Even more concerning was that the lesion was not well centered around the root apex and was localized around the lateral root surface. Frequently patients like this are told “This tooth is fractured, it has to come out” without even attempting endodontic treatment. This case presents a great […]
3 reasons why we have teeth
3 reasons why we have teeth
3 reasons why we have teeth: 1) Esthetics 2) Function: allows you to speak and eat 3) Stability: keeps other teeth from moving around. Bottom line? When you can’t save the tooth…replace it… […]
Emergency Tooth Replantation: Procedures, Success Rates & Risks
Emergency Tooth Replantation: Procedures, Success Rates & Risks
FIXING COMPROMISED CASES
FIXING COMPROMISED CASES
FIXING COMPROMISED CASES: This 50 y.o. healthy male presents with pain associated with the support tooth of his bridge. We have noted a 6 unit FPD with #5 and #6 used as pier abutments. We have diagnosed a recurrent infection associated with #6 secondary to a misplaced post causing a perforation on the disto-palatal aspect. As all potential options involving removal of the FPD would be very costly to replace, we made the decision to perform surgical repair of the perforated post. Root end preparation and retrofill was also done to seal off all potential communications from the canal system […]
INSTRUMENT REMOVAL
INSTRUMENT REMOVAL
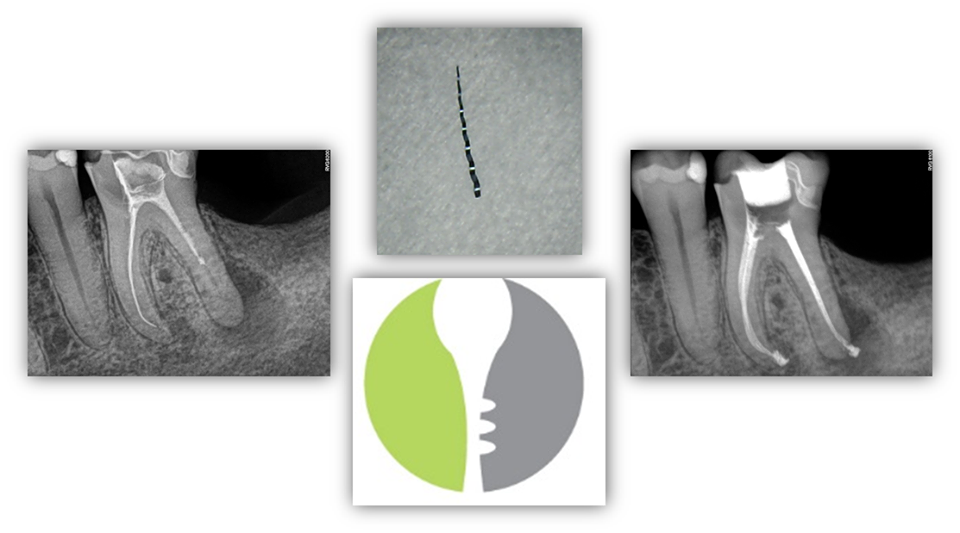
INSTRUMENT REMOVAL – This patient presented to our office with a previously initiated RCT #19 with a separated retained instrument in the ML canal. Information regarding “pathophysiology” of instrument separation, risk-benefit ratio of removing the retained instrument, alternative options if instrument removal cannot be achieved (i.e. bypass and/or apicoectomy), and prognosis were reviewed with the patient. The patient was motivated to save his tooth at all costs. Upon access, the retained instrument was visualized in the ML canal. The instrument was successfully removed using ultrasonics and hedstrom files. The patient was pleased with the final result. […]
TRANSIENT APICAL BREAKDOWN
TRANSIENT APICAL BREAKDOWN
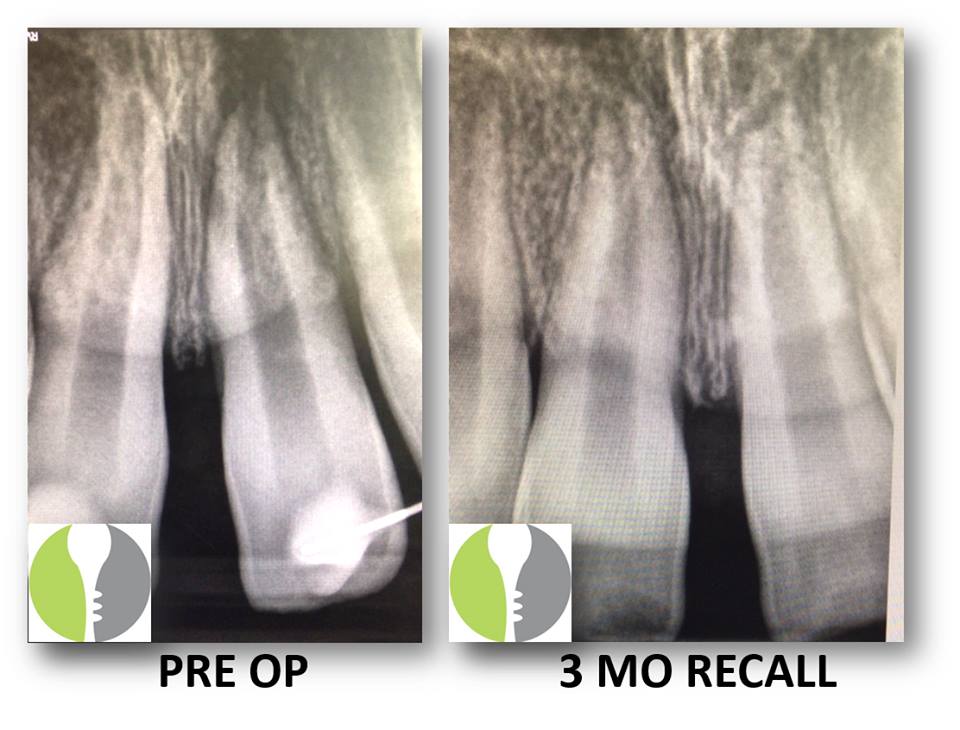
TRANSIENT APICAL BREAKDOWN: Here we present a case of a young healthy male who sustained facial trauma involving monkey bars and affecting tooth #9. He had subsequently had a splint placed at the ER to rectify a subluxation injury and was referred to our office for follow-up and necessary treatment. Upon initial evaluation, the tooth was still slightl symptomatic and tested negatively to pulp vitality testing. Additionally, there appeared to be a lesion on radiograph. As the traumatic incident was recent, we recommended that the tooth be re-evaluated at a future date (in this case 3 months) and instructed the […]
COMPROMISED CASES
COMPROMISED CASES
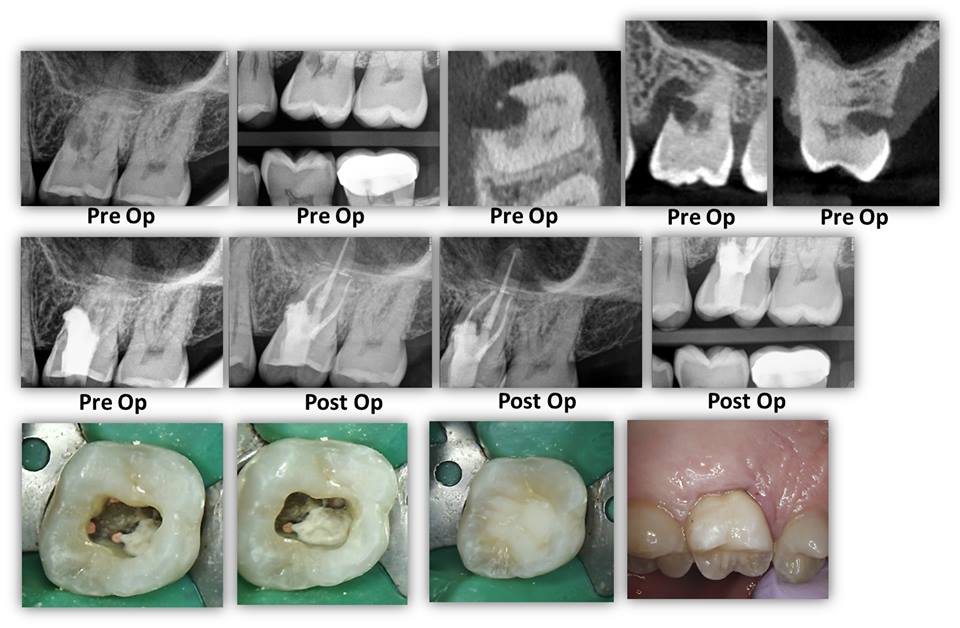
COMPROMISED CASES: Here we present a case where both restorative dentist and periodontist were a little unsure as to what could be done here with regards to the large resorption defect on the mesio-palatal aspect. Periodontal surgery was initially in the plan should the tooth be deemed restorable. We deconstructed the case via complete canal instrumentation, degranulation of the resorption defect, and medication with Ca[OH]2. On the second visit, we completed the root canal and repaired the defect with Brasseler Root Repair Material and sealed it with a dual cured core composite. At 8 weeks between treatment initiation and completion, the […]
Endodontist Competency in Implant Dentistry
Should my Endodontist to be Competent in Implants?
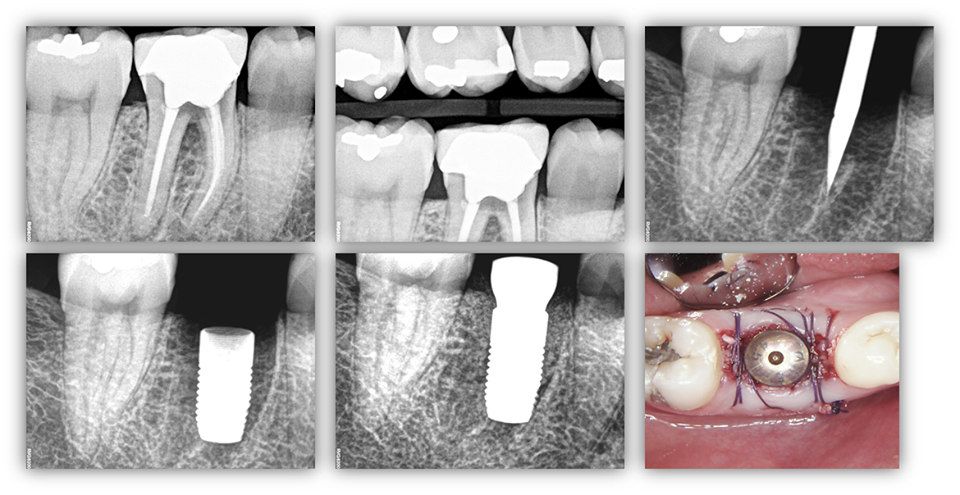
IS IT BENEFICIAL FOR YOUR ENDODONTIST TO BE COMPETENT IN IMPLANT DENTISTRY? Here we present a patient that was referred to our office for “retreatment” of tooth #30. Upon radiographic survey and clinical evaluation, the tooth was deemed non-restorable primarily due to recurrent decay in the furcation area causing a secondary bone loss. To ensure that this tooth was the only significant dental need, communication was made both to ensure adequate interoffice communication (i.e. approval) and to ensure that there is no other dental needs of higher priority. After being given the greenlight to proceed with the procedure, extraction was […]
Read More… from Should my Endodontist to be Competent in Implants?
A Patient's Guide to Apicoectomy
A Patient’s Guide to Apicoectomy
