HOPELESS PROGNOSIS?: Based on the pre-operative PA, many dentists would suggest to their patients that this tooth has a poor or hopeless prognosis. Clinically it had a 12 mm probing to the apex and radiographically it has a large apical lesion that was confirmed to extend around the entire MB root on CBCT. Even more concerning was that the lesion was not well centered around the root apex and was localized around the lateral root surface. Frequently patients like this are told “This tooth is fractured, it has to come out” without even attempting endodontic treatment. This case presents a great […]
Tag: CBCT
HOPELESS PROGNOSIS?
Emergency Tooth Replantation: Procedures, Success Rates & Risks
Emergency Tooth Replantation: Procedures, Success Rates & Risks
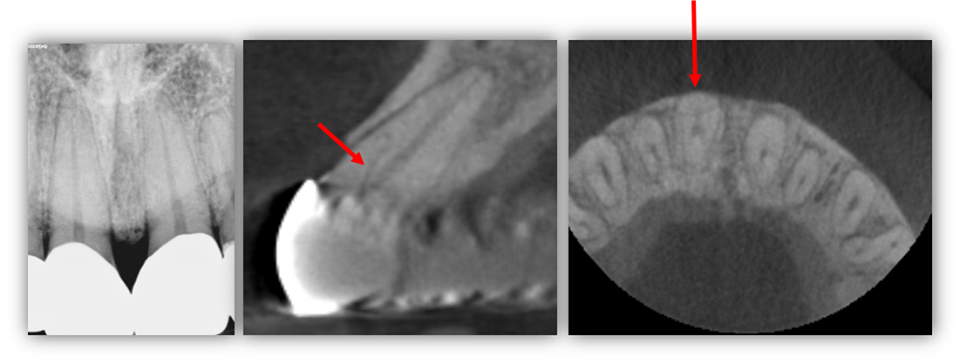
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT – Typically, a crack cannot be identified on a CBCT scan unless the crack is large. In this case a patient presented with a large MOD crack of tooth #15. The crack was large enough that an explorer could be inserted and the buccal and palatal segments agitated. CBCT was exposed and the MOD crack can be visualized to its terminus on the palatal aspect of the MB root. Here, CBCT was a great tool for diagnosis, prognosis, and patient education. […]
Treatment Planning Dilemmas
TREATMENT PLANNING DILEMMAS
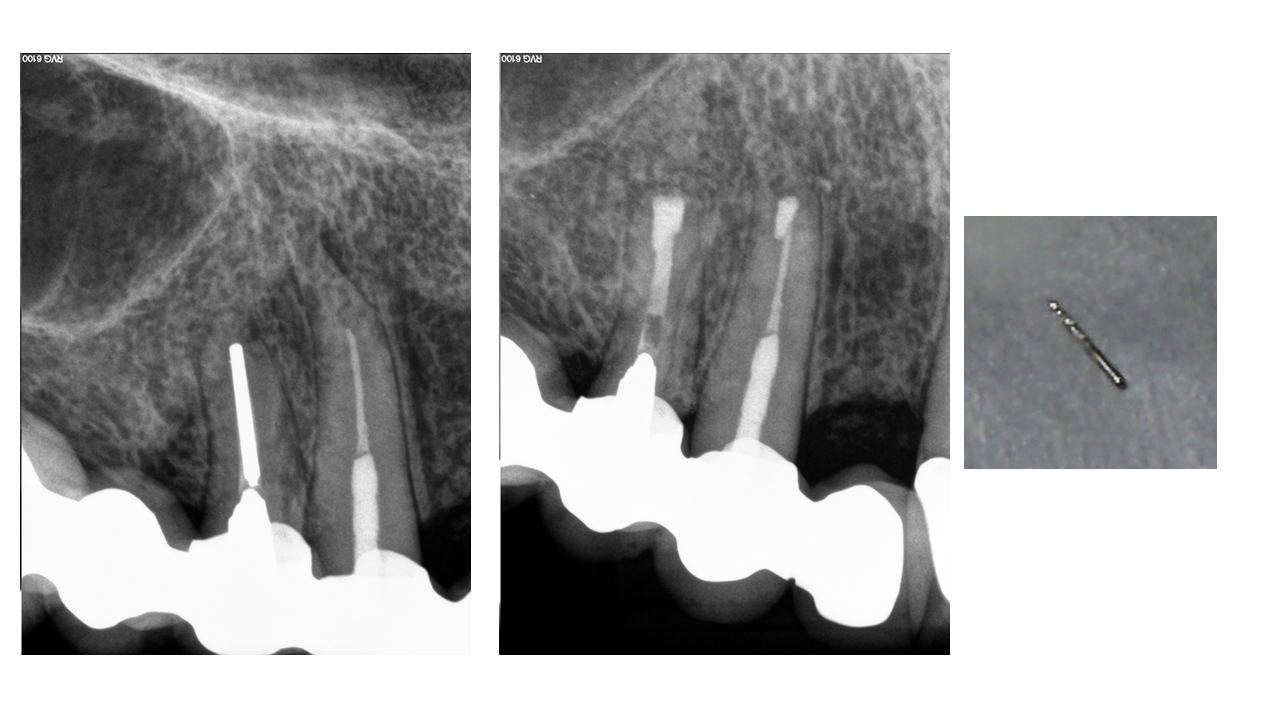
TREATMENT PLANNING DILEMMAS: Here we present a case with an initial presentation of a history of both non-surgical and surgical treatment (of the MB root). The patient’s chief complain included persistent pain. CBCT (not shown here) confirmed a lesion associated with the MB root. Interestingly, we also noted that surgery had been done on the MB canal but not he MB2 canal due to an incomplete root resection. The apical plug associated with the MB canal was intact. With the help of the patient’s lack of motivation to pursue surgery again, the decision was made to non-surgically retreat the case. One […]
What You Didn't Know About Molar Anatomy
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY

WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY CBCT is slowly becoming the standard of care for endodontics for many reasons. In a tooth with a somewhat unusual root shape, such as the case demonstrated here, CBCT helps us determine the number of canals so that we can keep our accesses minimal and make informed decisions of where to look for accessory canals such as an MB2. This tooth had a conical root shape so a CBCT was taken to determine anatomy. As you can see below, this is a highly unusual anatomy where the DB root bifurcates to form four […]
An Unusual 'Post' Removal
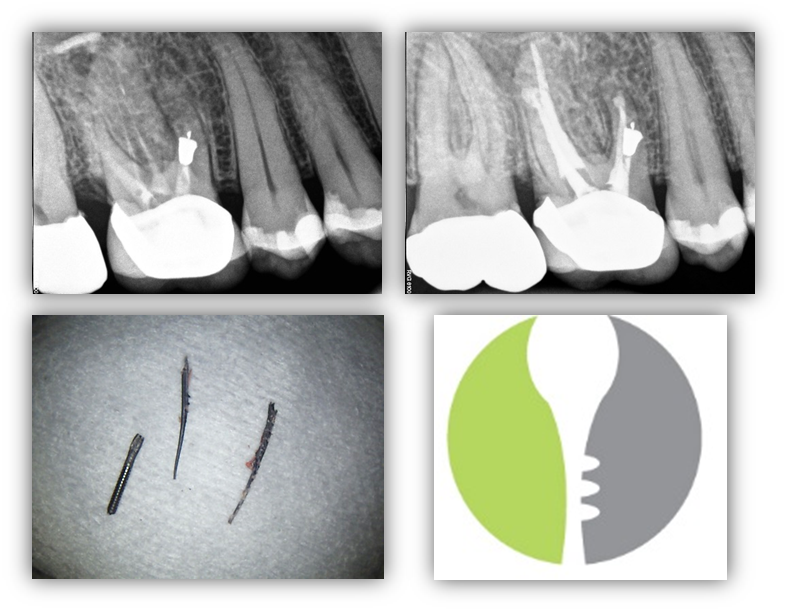
AN UNUSUAL ‘POST’ REMOVAL
AN UNUSUAL ‘POST’ REMOVAL Apicoectomy can be a highly predictable treatment option for patients with failing endodontic therapy. Modern microscurgery involves not only root resection, but also retropreparation using ultrasonics and retrofil using bioceramic materials like MTA. Without these two key factors, treatment success drops from ~87% to nearly 60% and is the reason apicoectomy tends to have a “50/50” connotation with some oral surgeon offices. The following is a great case to demonstrate the possibilities in modern endo! Pre-operatively you can note that the ‘post’ (silver point) goes to the apex and CBCT showed a corresponding lesion. Placing bioceramics on […]
Why is it Beneficial for Endodontists to be Proficient in Extractions and Socket Preservation?
WHY IS IT BENEFICIAL FOR ENDODONTISTS TO BE PROFICIENT IN EXTRACTIONS AND SOCKET PRESERVATION?
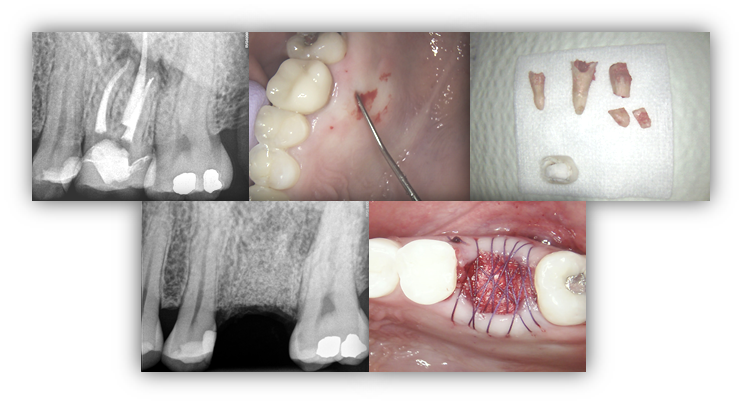
WHY IS IT BENEFICIAL FOR ENDODONTISTS TO BE PROFICIENT IN EXTRACTIONS AND SOCKET PRESERVATION? This patient presented to our office complaining of a draining sinus tract on the palatal gingiva of tooth #14. Clinically, tooth #14 had an isolated deep probing depth of 13mm on the palatal aspect with corresponding complete bone loss around the palatal root on the CBCT (not pictured below). The patient was advised that these findings are consistent with vertical root fracture and prognosis is hopeless. The patient was highly motivated to extract tooth #14 and restore with an implant. Although it is not a requirement […]
Persistent Pain Following RCT
PERSISTENT PAIN FOLLOWING RCT
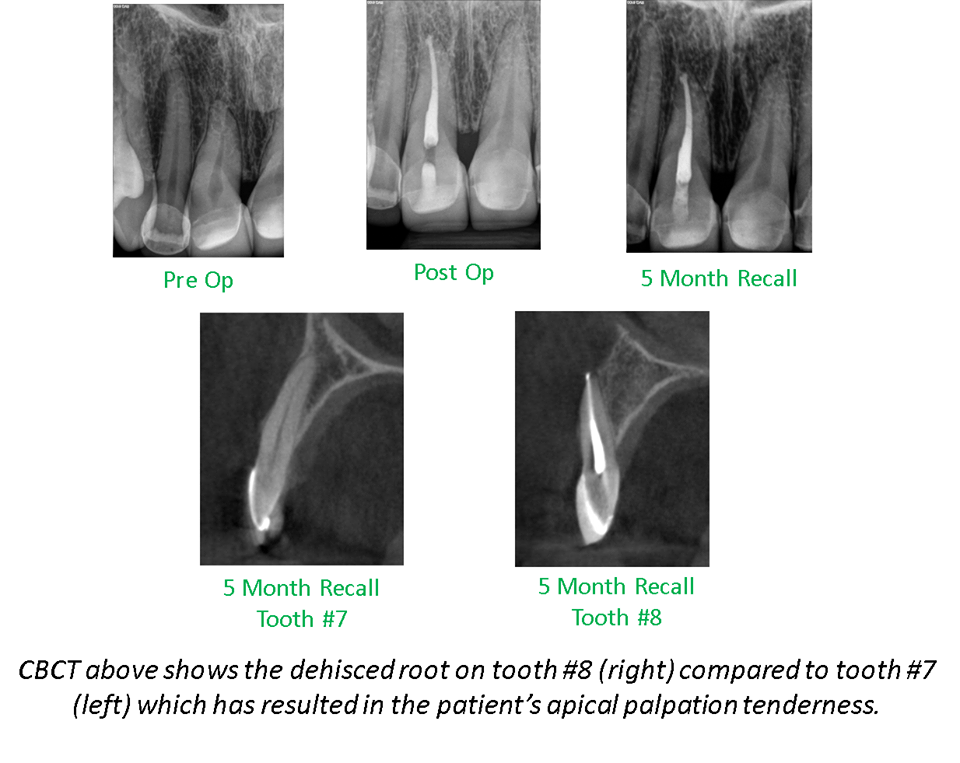
PERSISTENT PAIN FOLLOWING RCT: Determining the etiology of persistent pain following a “well-done root canal” can be a challenge as there are many possible explanations. Such possibilities include an untreated canal, coronal leakage, fracture, or referred pain from another tooth or non-odontogenic structure. The attached images are of a 41 year-old patient who returned to our office 5 months following RCT tooth #8. The patient described her “persistent pain” as tenderness when she palpates the facial gingiva overlying apex #8. CBCT examination demonstrated that tooth #8 is facially inclined with its apex located outside of the bony housing of the maxilla—allowing […]
Endodontic Treatment Planning Dilemmas
ENDODONTIC TREATMENT PLANNING DILEMMAS

ENDODONTIC TREATMENT PLANNING DILEMMAS: Here we present an interesting case of a 47yo healthy Asian male with an exceptionally esthetic FPD #3-5 with #4 as the pier abutment. The FPD was done a little over a year prior to initial presentation to our office. The patient had subsequently presented to our office with persistent bite discomfort and pain upon digital palation of the “gums”. Although both #4 and #5 were infected, #4 had a vertical root fracture traveling from the apical –> coronal (confirmed via CBCT and subsequent surgical access). Apical surgery was initially planned on #5 and full root […]
Trauma and CBCT
TRAUMA AND CBCT
TRAUMA AND CBCT: Yet another trauma case where CBCT evaluation was an integral part of diagnosis and treatment planning. This patient presented to our office two days after taking an elbow to the mouth during a volleyball match. The patient stated immediately following the incident, he noted bleeding of the gingival sulcus and pain tooth #8. He denied tooth movement or malpositioning. Tooth #8 had a full coverage crown, was tender to percussion and palpation, Class III mobility, no response to cold, no isolated deep probing depths, and widened PDL space in the apical third. Teeth #6, 7, 9, 10, and […]