[…]
UNUSUAL PRESENTATION OF A ROOT FRACTURE

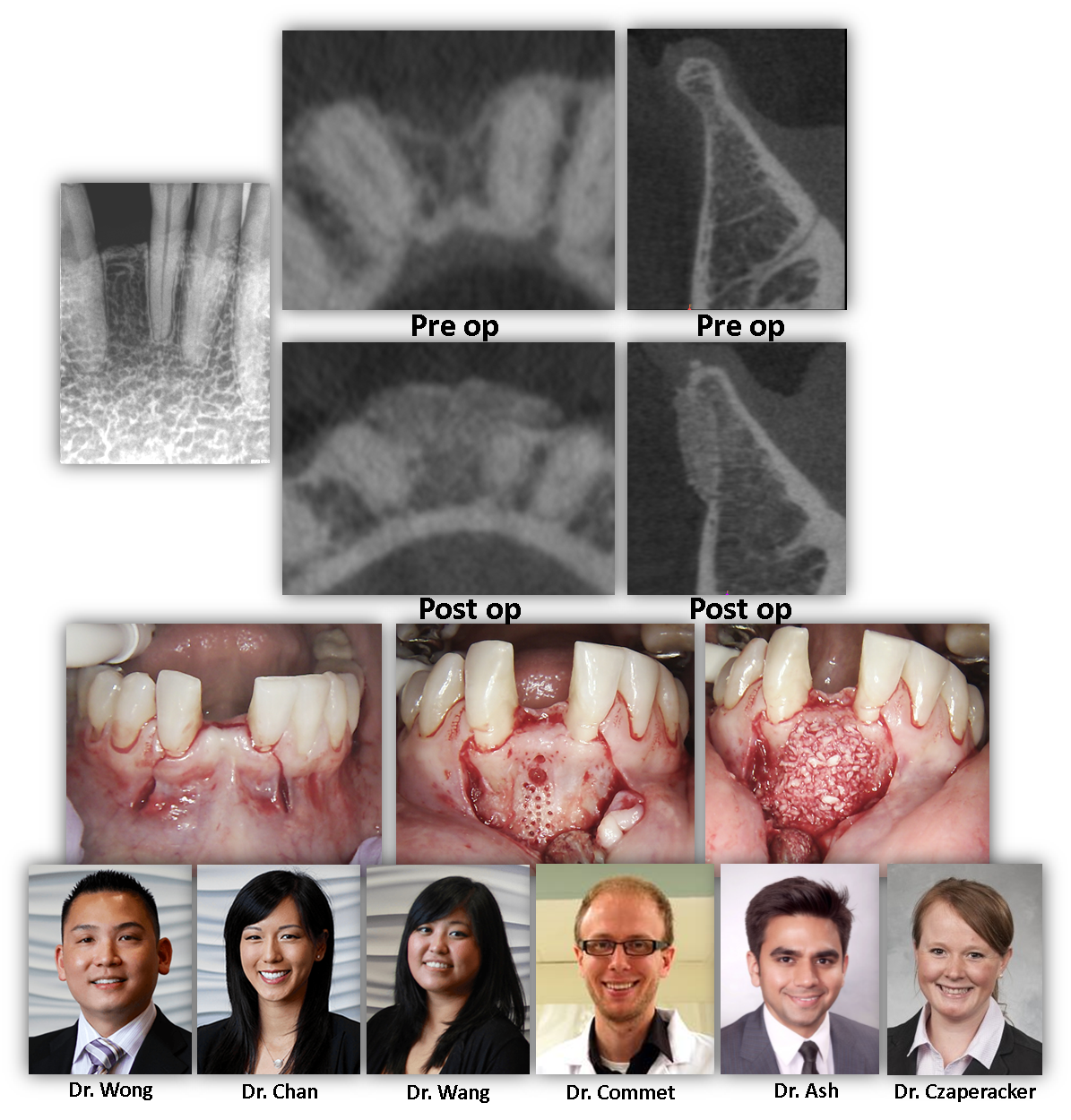
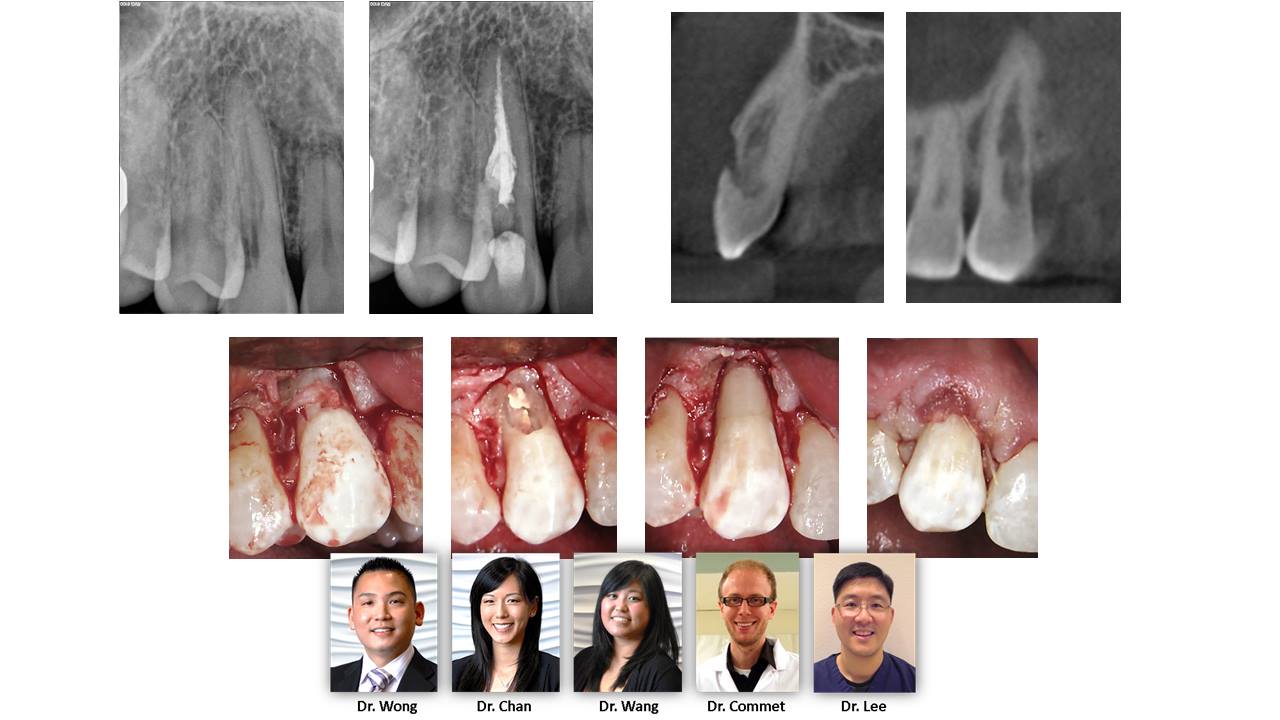
INVASIVE CERVICAL RESORPTION PART 2: Another interesting example of a compromised anterior tooth that came through the office. This one has class Hiethersay Class IV (resorption into the root structure), but with careful planning using CBCT and surgical therapy, a great outcome can be achieved. Stay tuned for “Invasive Cervical Resorption Part 3: Return of the Tooth Jedi” […]
Read More… from Understanding Invasive Cervical Resorption: Causes, Symptoms, and Treatment
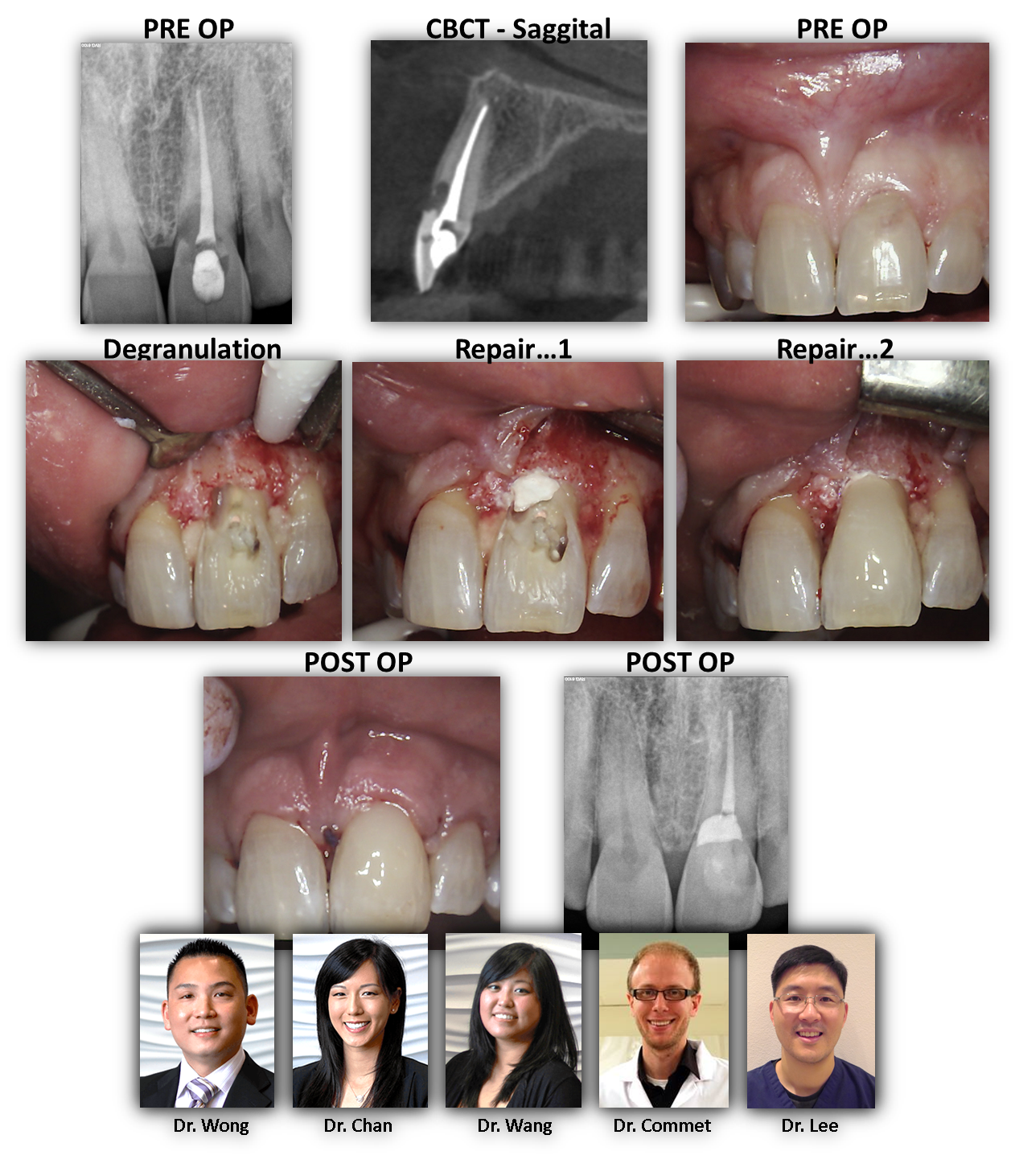
INVASIVE CERVICAL RESORPTION: Here is an interesting case. This patient ended up in our care after a root canal was done on tooth #9. He was informed at that time that it wasn’t guaranteed that the tooth could be saved and that a dental implant might be necessary or a surgery of some sort. As one can see on the pre-operative radiographs, sagittal slice of the CBCT and clinical photo, there is clear evidence of invasive cervical resorption on the buccal aspecdt extending below… the level of the crest. Additionally, the granulation tissue was not addressed via non-surgical access. Because […]
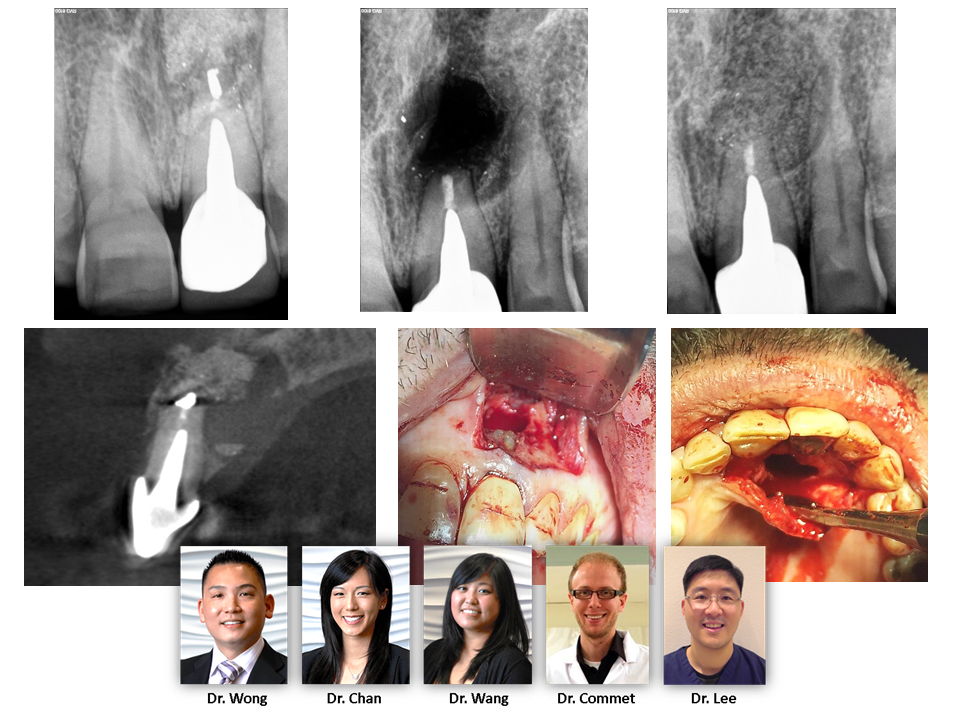
CBCT IMAGING – As many of us are aware, CBCT imaging applications for dentistry are growing at an exponential rate. This case highlights an unusual scenario where the patient received an apicoectomy on tooth #9 ~25 years prior to presentation. His chief complaint was a large sinus tract that had recently developed. Convential PA shows a moderate diameter lucency around the root apex. However, the …CBCT volume highlights an existing osseous graft (later revealed to be bovine bone graft through histology) that is infected and encapsulated by soft tissue. The native bone destruction is actually quite large and perforated on […]

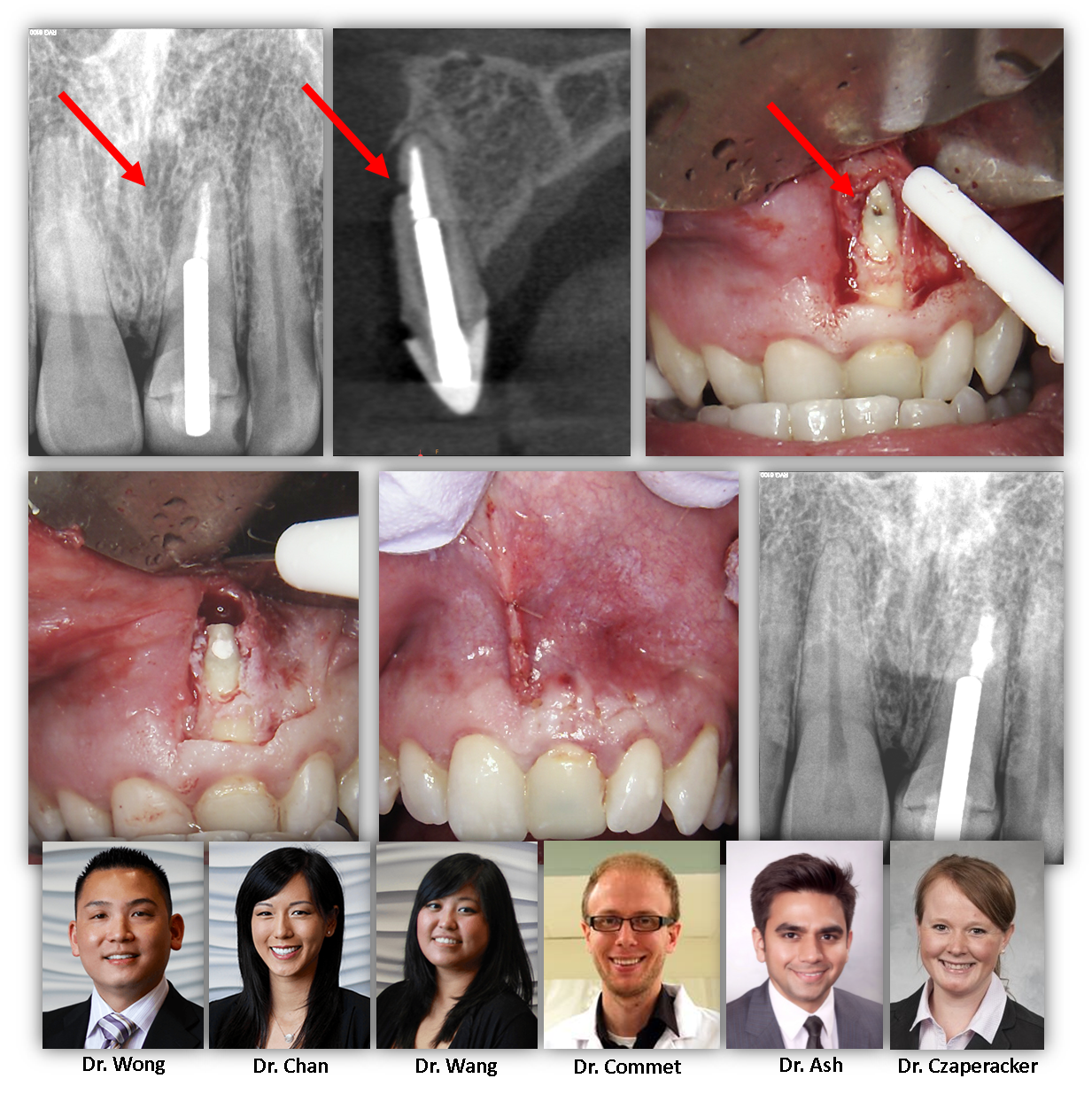
Here is a 79yo healthy female with non-remarkable medical history. She presented with a history of massive palatal swelling due to perforation of the palatal root from attempted retreatment by her dentist. As you can see, a part of the previous casted post remains in the palatal root. We have identified the perforation on 2D imaging and confirmed with CBCT (we area aware of an untreated MB2 canal; however, there is no evidence of periapical pathology and retreatment will not be attempted until we can confirm that we have rectifed the palatal pathology). We have decided to attempt repairing the […]

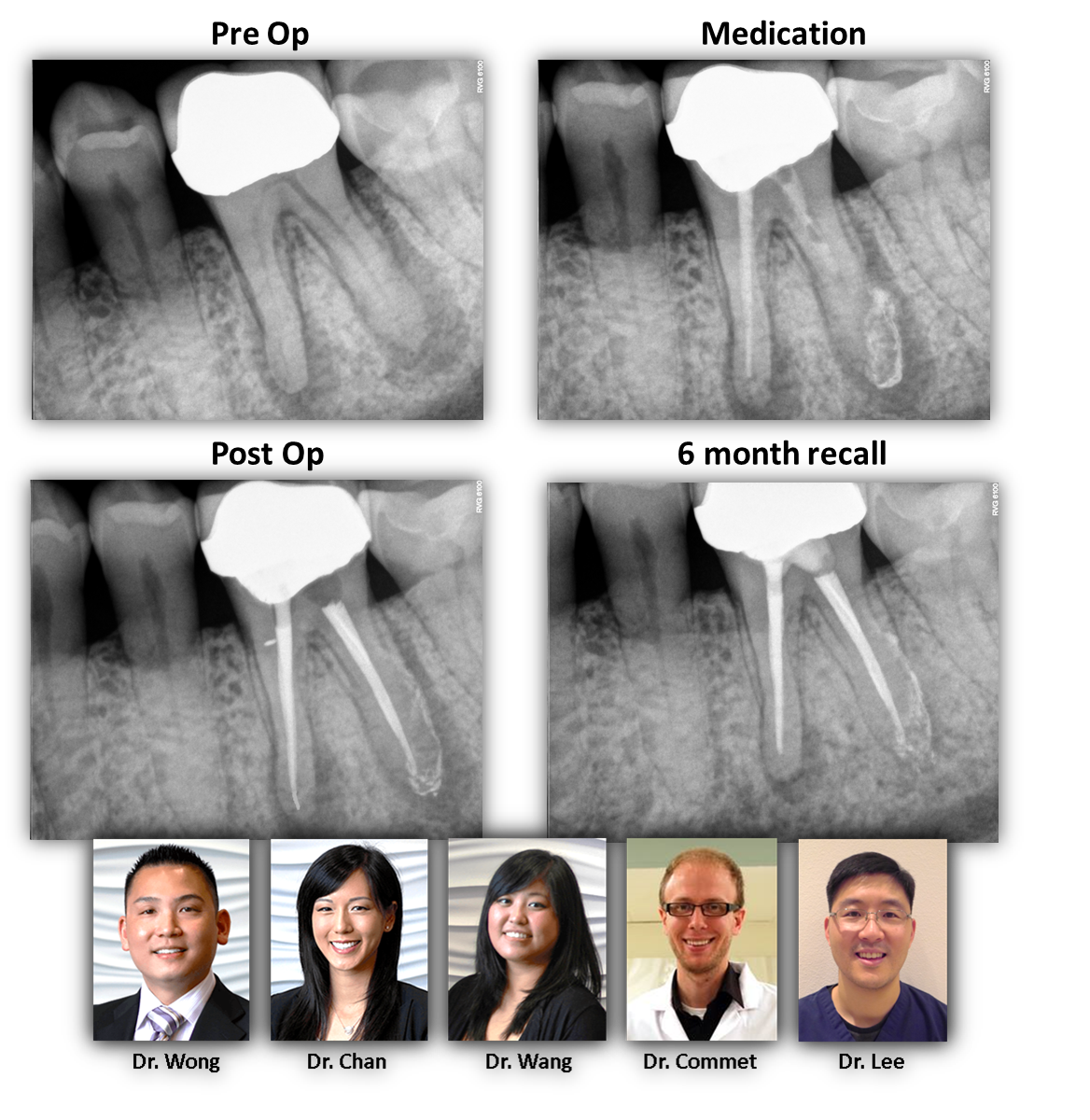
This case was referred to our office for evaluation and expected extraction with eventual dental implant. Radiographically there was a large lesion associated with the mesial root, accompanying deep probing, and large swelling at the gingival margin. This case has several signs that would be consistent with non-restorable fracture. However, we used all available diagnostic tools, including CBCT, and could not definitively identify a fracture that would condemn the tooth to extraction. Therefore, we pursued retreatment with 6 weeks intracanal medicament. At the time of case completion, this patient was completely asymptomatic and the gingival tissue was healthy and firm. […]