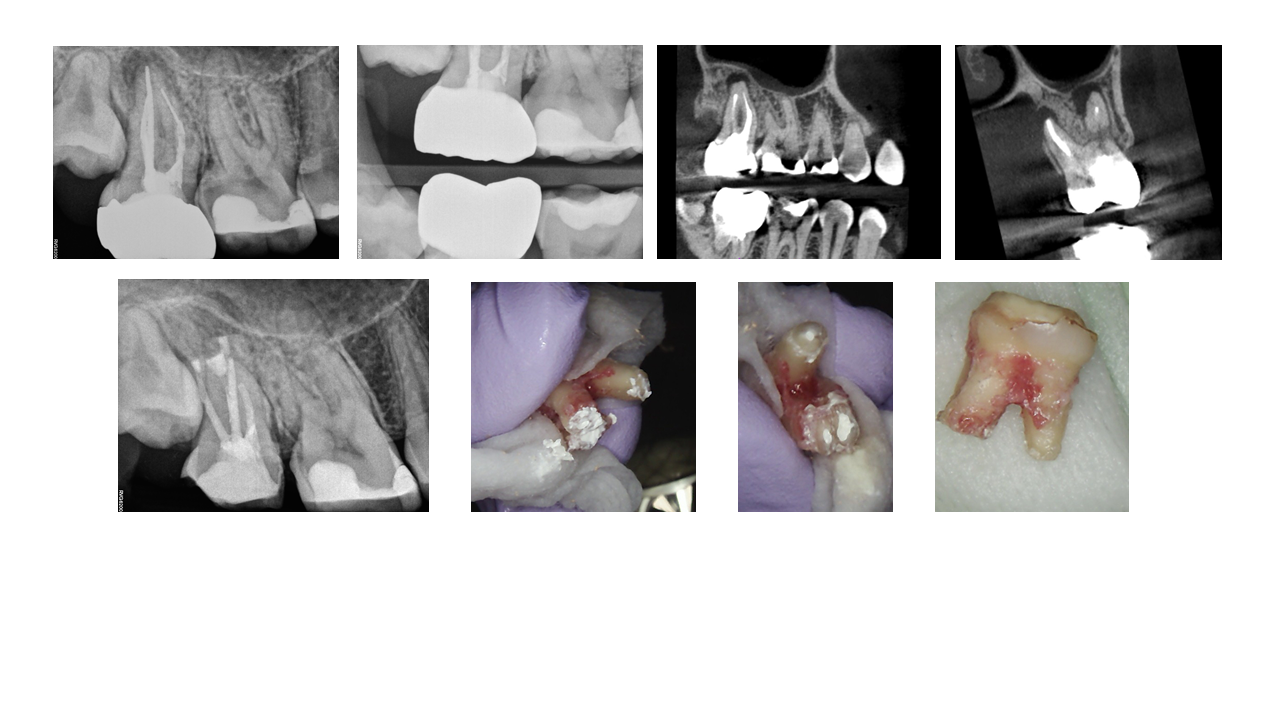
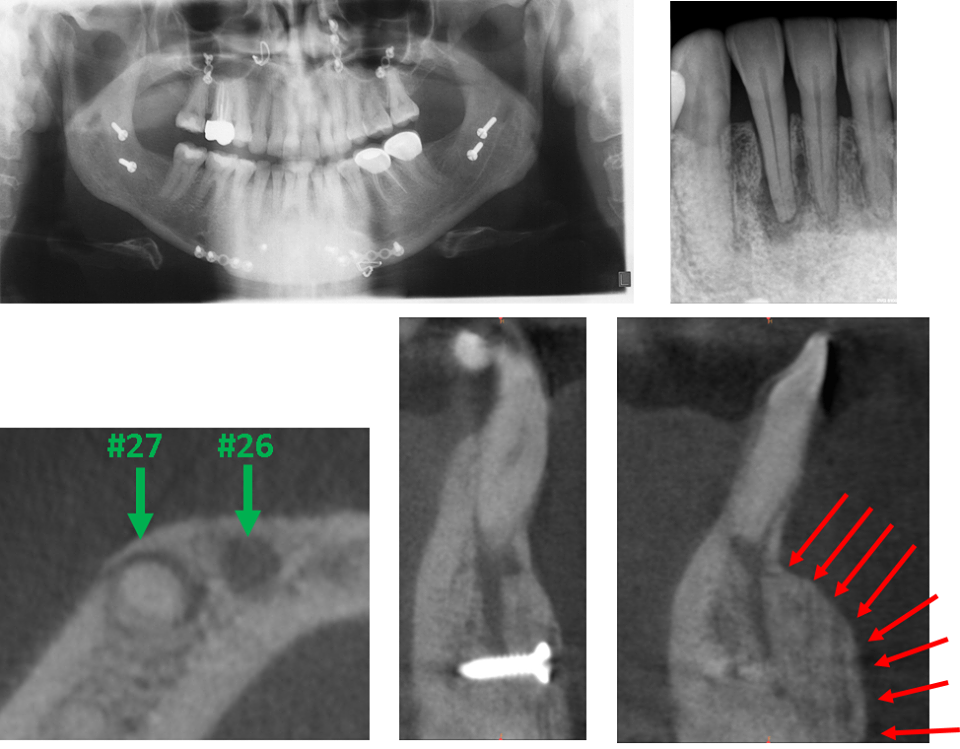
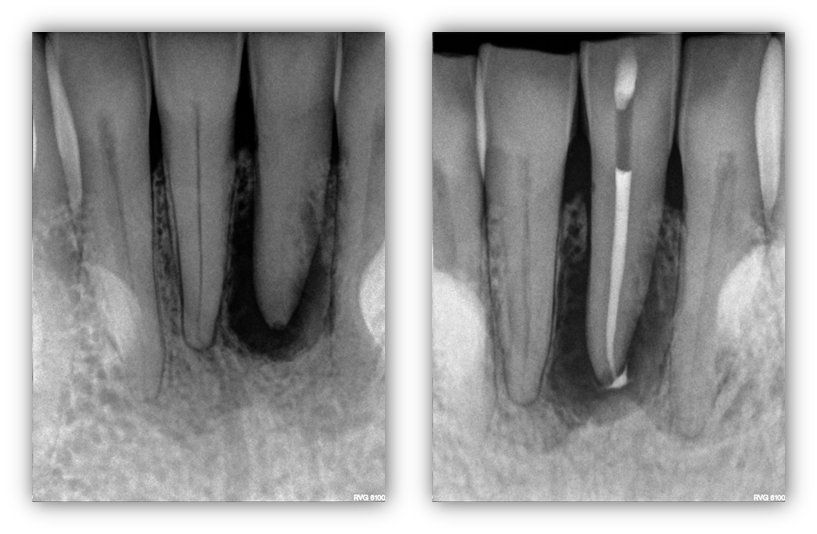
ENDODONTIC TREATMENT PLANNING DILEMMAS: Here we present an interesting case of a 47yo healthy Asian male with an exceptionally esthetic FPD #3-5 with #4 as the pier abutment. The FPD was done a little over a year prior to initial presentation to our office. The patient had subsequently presented to our office with persistent bite discomfort and pain upon digital palation of the “gums”. Although both #4 and #5 were infected, #4 had a vertical root fracture traveling from the apical –> coronal (confirmed via CBCT and subsequent surgical access). Apical surgery was initially planned on #5 and full root […]
ENDODONTIC TREATMENT PLANNING DILEMMAS