[…]
Read More… from Dental Trauma in Adults: What to Do If You Crack or Lose a Tooth
HOPELESS PROGNOSIS?: Based on the pre-operative PA, many dentists would suggest to their patients that this tooth has a poor or hopeless prognosis. Clinically it had a 12 mm probing to the apex and radiographically it has a large apical lesion that was confirmed to extend around the entire MB root on CBCT. Even more concerning was that the lesion was not well centered around the root apex and was localized around the lateral root surface. Frequently patients like this are told “This tooth is fractured, it has to come out” without even attempting endodontic treatment. This case presents a great […]
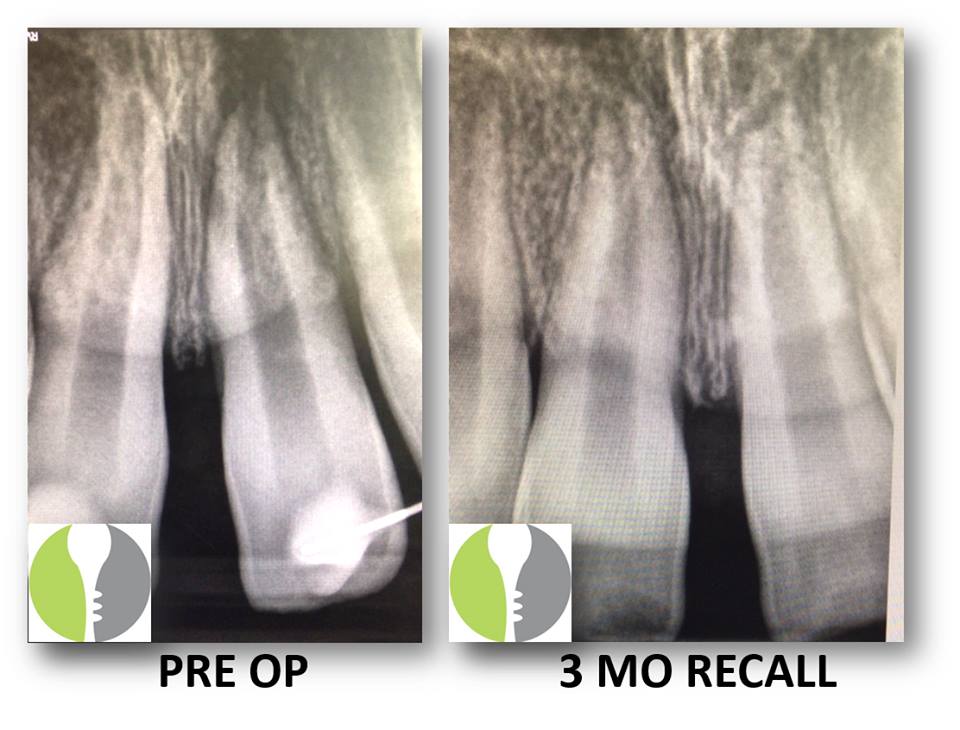
TRANSIENT APICAL BREAKDOWN: Here we present a case of a young healthy male who sustained facial trauma involving monkey bars and affecting tooth #9. He had subsequently had a splint placed at the ER to rectify a subluxation injury and was referred to our office for follow-up and necessary treatment. Upon initial evaluation, the tooth was still slightl symptomatic and tested negatively to pulp vitality testing. Additionally, there appeared to be a lesion on radiograph. As the traumatic incident was recent, we recommended that the tooth be re-evaluated at a future date (in this case 3 months) and instructed the […]
COMPROMISED CASES: Here we present a case where both restorative dentist and periodontist were a little unsure as to what could be done here with regards to the large resorption defect on the mesio-palatal aspect. Periodontal surgery was initially in the plan should the tooth be deemed restorable. We deconstructed the case via complete canal instrumentation, degranulation of the resorption defect, and medication with Ca[OH]2. On the second visit, we completed the root canal and repaired the defect with Brasseler Root Repair Material and sealed it with a dual cured core composite. At 8 weeks between treatment initiation and completion, the […]
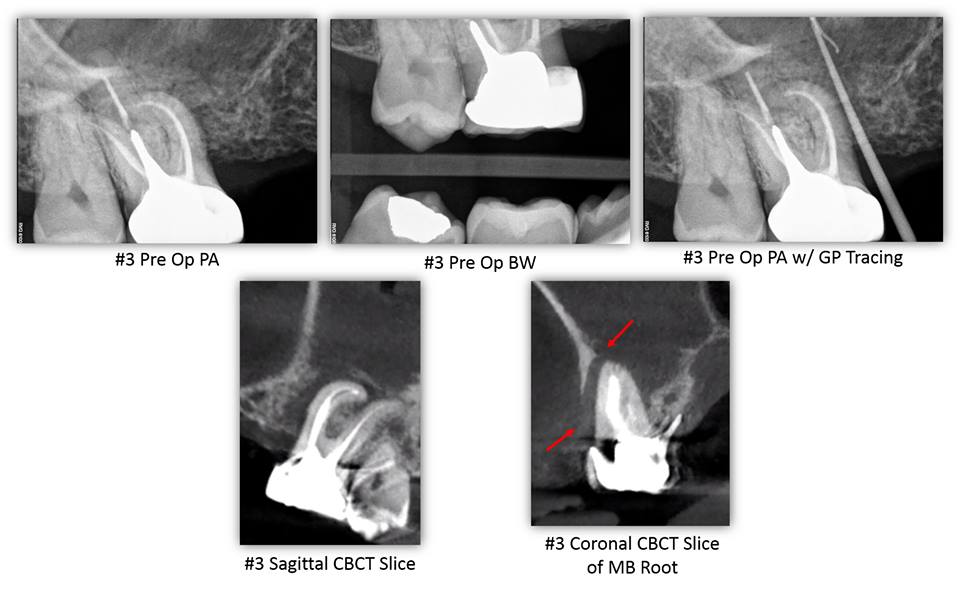
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY– This patient presented for evaluation of tooth #3. His chief complaint was a painful swelling of gum that would sometimes bleed in the area of tooth #3. The patient reported RCT #3 was completed over 20 years ago by an Endodontist. The patient stated that he is congenitally missing teeth #4, 5, 12, and 13. The patient denies wearing an RPD. The patient’s chief complaint was consistent with a sinus tract located mesial to tooth #3 at the level of the alveolar crest. The sinus tract was traced with gutta-percha. Tooth #3 had an intact […]
Read More… from OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
CRACK EXTENSION DETERMINED BY CBCT – Typically, a crack cannot be identified on a CBCT scan unless the crack is large. In this case a patient presented with a large MOD crack of tooth #15. The crack was large enough that an explorer could be inserted and the buccal and palatal segments agitated. CBCT was exposed and the MOD crack can be visualized to its terminus on the palatal aspect of the MB root. Here, CBCT was a great tool for diagnosis, prognosis, and patient education. […]
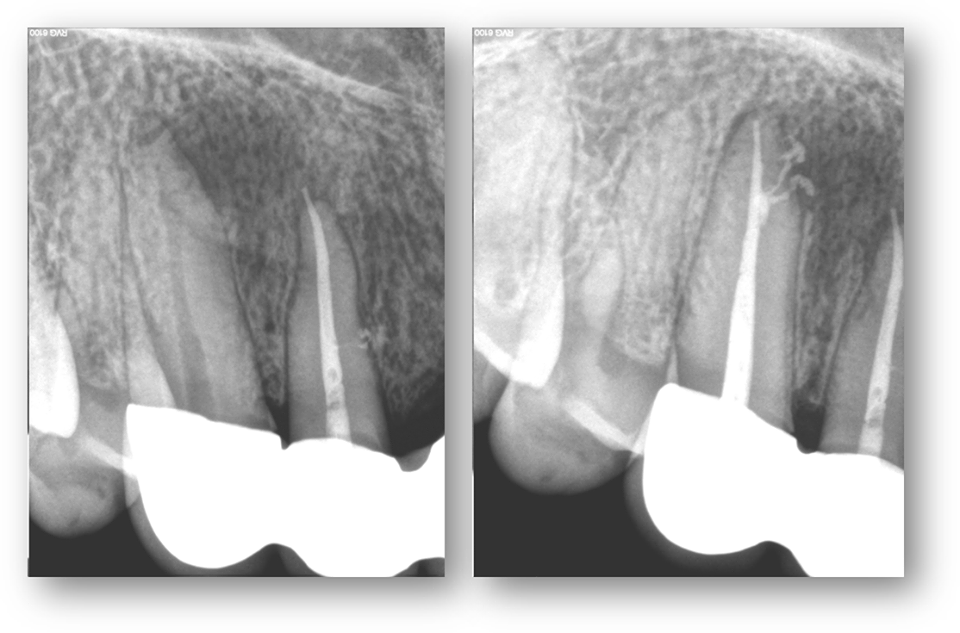
LESION SHAPE SUGGESTIVE OF ROOT CANAL ANATOMY: This is a pretty good demonstration of periapical lesion associated with the canine tooth (#6). Pre-operative radiographic survey reveals that the lesion is off to the side at the apical third. Post-operative radiograph highlights a couple accessory canals providing a route of infection and inflammatory response in the area of the lesion. Good demonstration of anatomy here. […]
Read More… from LESION SHAPE SUGGESTIVE OF ROOT CANAL ANATOMY

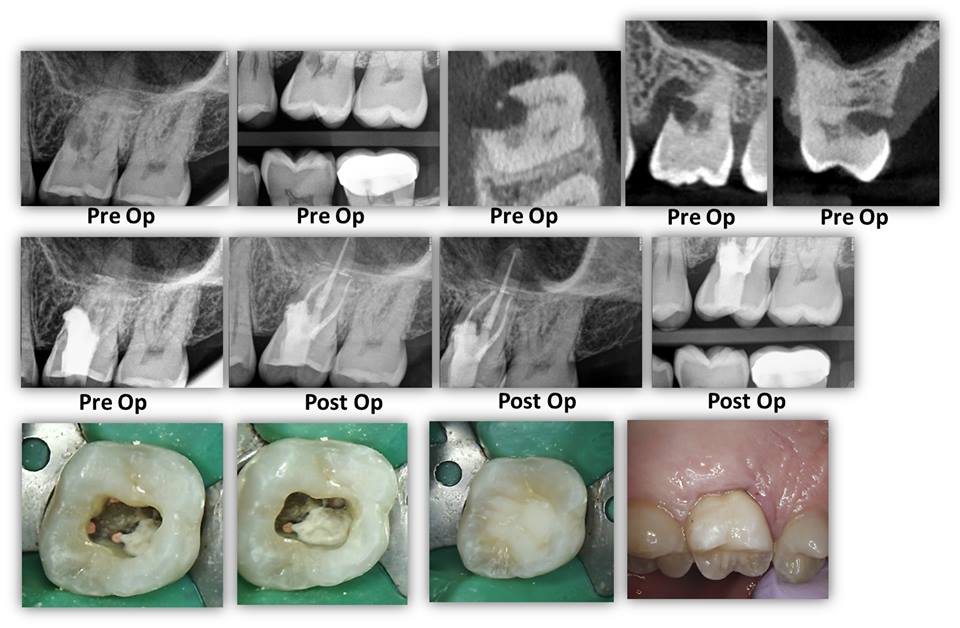
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY CBCT is slowly becoming the standard of care for endodontics for many reasons. In a tooth with a somewhat unusual root shape, such as the case demonstrated here, CBCT helps us determine the number of canals so that we can keep our accesses minimal and make informed decisions of where to look for accessory canals such as an MB2. This tooth had a conical root shape so a CBCT was taken to determine anatomy. As you can see below, this is a highly unusual anatomy where the DB root bifurcates to form four […]