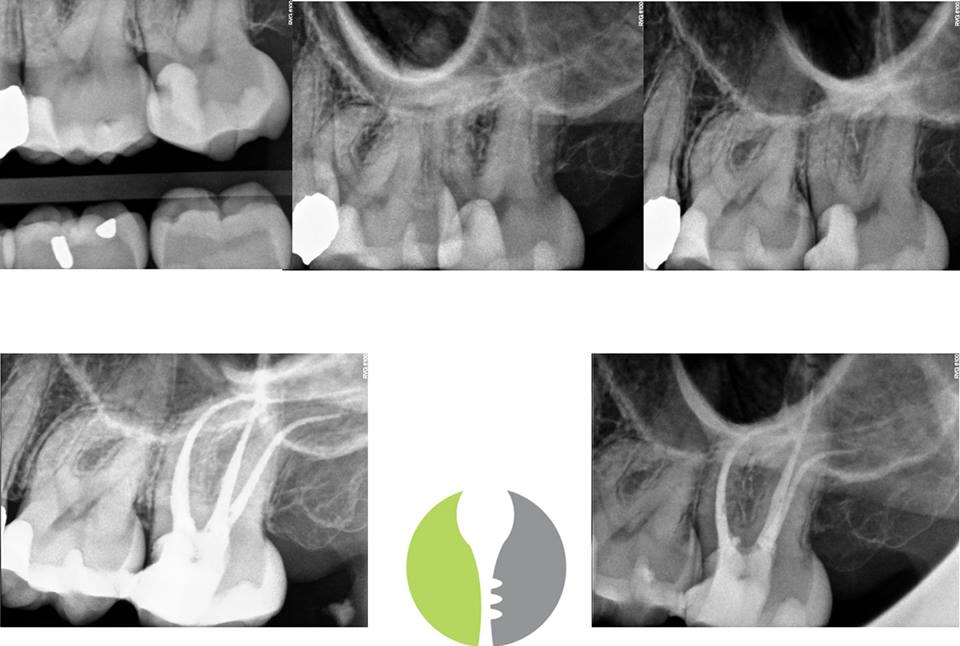
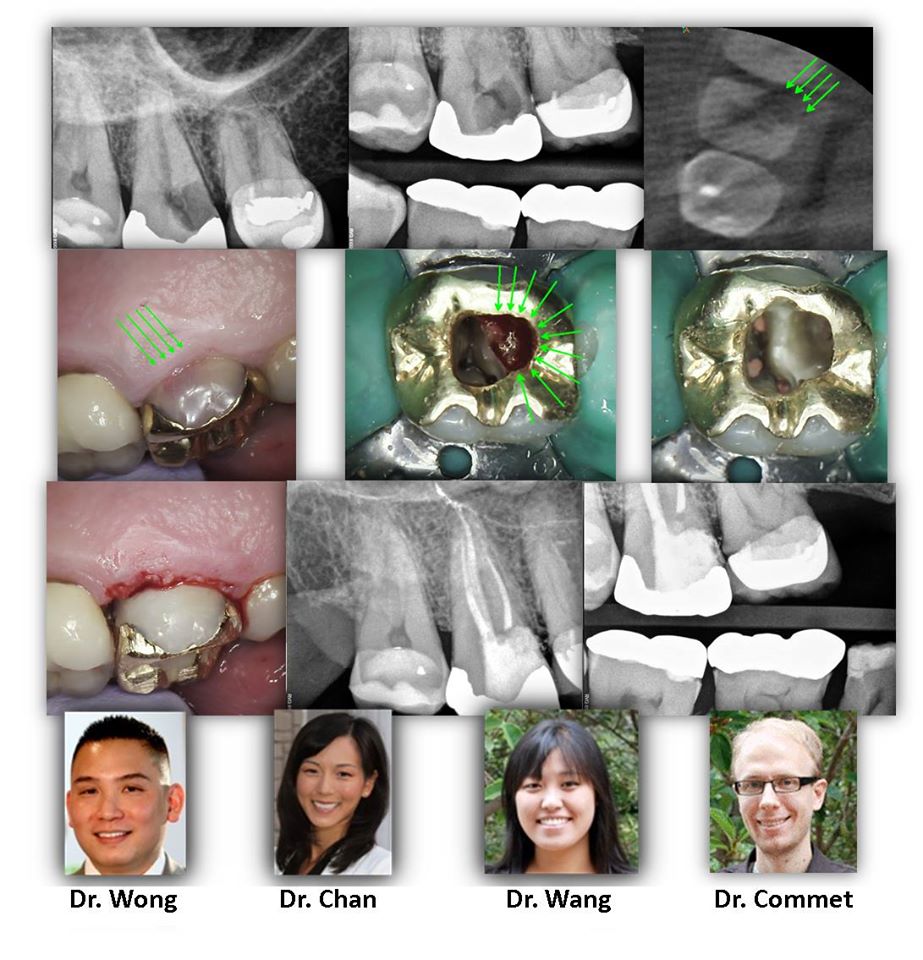
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY CBCT is slowly becoming the standard of care for endodontics for many reasons. In a tooth with a somewhat unusual root shape, such as the case demonstrated here, CBCT helps us determine the number of canals so that we can keep our accesses minimal and make informed decisions of where to look for accessory canals such as an MB2. This tooth had a conical root shape so a CBCT was taken to determine anatomy. As you can see below, this is a highly unusual anatomy where the DB root bifurcates to form four […]
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY