HOPELESS PROGNOSIS?: Based on the pre-operative PA, many dentists would suggest to their patients that this tooth has a poor or hopeless prognosis. Clinically it had a 12 mm probing to the apex and radiographically it has a large apical lesion that was confirmed to extend around the entire MB root on CBCT. Even more concerning was that the lesion was not well centered around the root apex and was localized around the lateral root surface. Frequently patients like this are told “This tooth is fractured, it has to come out” without even attempting endodontic treatment. This case presents a great […]
Tag: MB
HOPELESS PROGNOSIS?
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
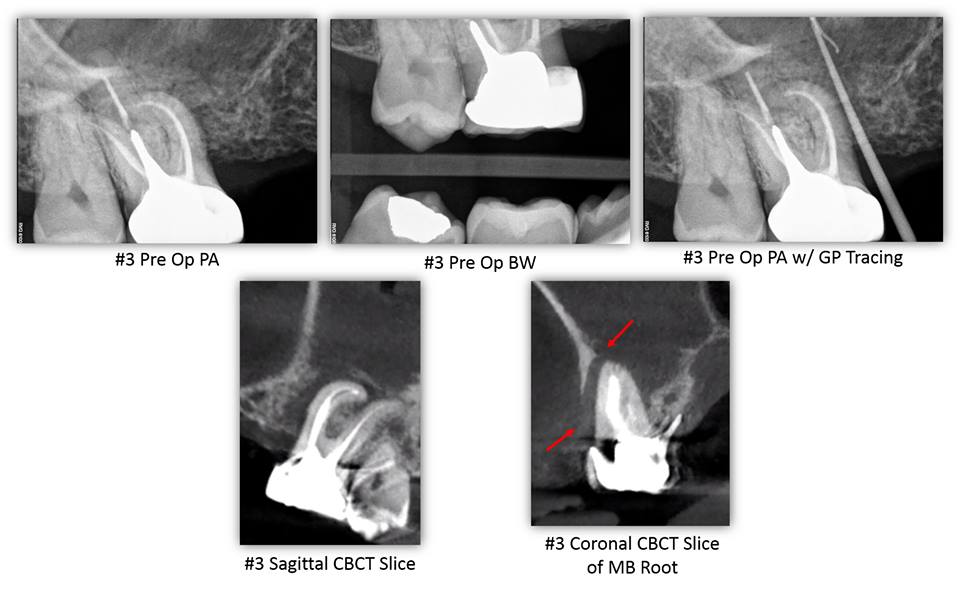
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY– This patient presented for evaluation of tooth #3. His chief complaint was a painful swelling of gum that would sometimes bleed in the area of tooth #3. The patient reported RCT #3 was completed over 20 years ago by an Endodontist. The patient stated that he is congenitally missing teeth #4, 5, 12, and 13. The patient denies wearing an RPD. The patient’s chief complaint was consistent with a sinus tract located mesial to tooth #3 at the level of the alveolar crest. The sinus tract was traced with gutta-percha. Tooth #3 had an intact […]
Read More… from OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT – Typically, a crack cannot be identified on a CBCT scan unless the crack is large. In this case a patient presented with a large MOD crack of tooth #15. The crack was large enough that an explorer could be inserted and the buccal and palatal segments agitated. CBCT was exposed and the MOD crack can be visualized to its terminus on the palatal aspect of the MB root. Here, CBCT was a great tool for diagnosis, prognosis, and patient education. […]
Treatment Planning Dilemmas
TREATMENT PLANNING DILEMMAS
TREATMENT PLANNING DILEMMAS: Here we present a case with an initial presentation of a history of both non-surgical and surgical treatment (of the MB root). The patient’s chief complain included persistent pain. CBCT (not shown here) confirmed a lesion associated with the MB root. Interestingly, we also noted that surgery had been done on the MB canal but not he MB2 canal due to an incomplete root resection. The apical plug associated with the MB canal was intact. With the help of the patient’s lack of motivation to pursue surgery again, the decision was made to non-surgically retreat the case. One […]
What You Didn't Know About Molar Anatomy
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY

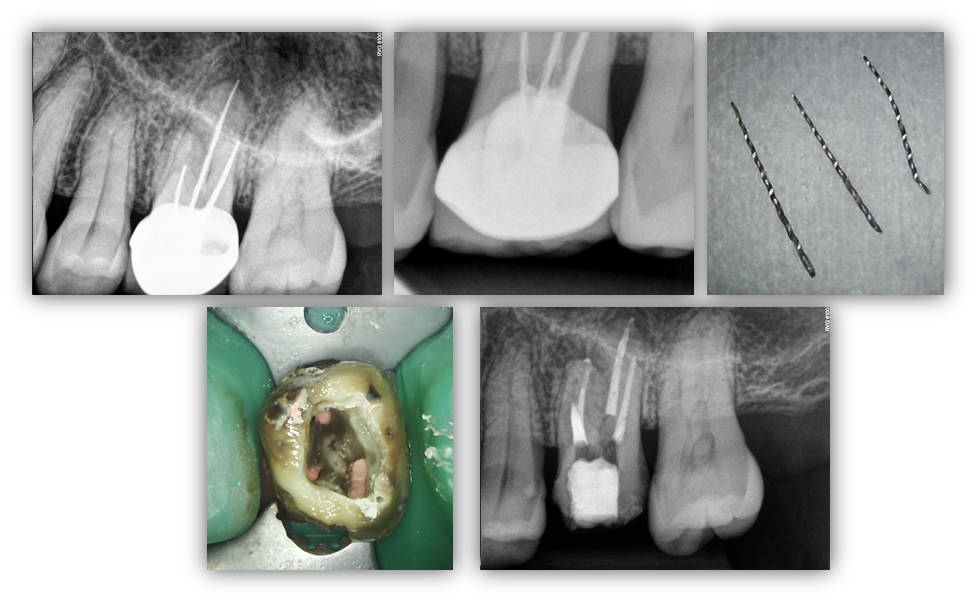
WHAT YOU DIDN’T KNOW ABOUT MOLAR ANATOMY CBCT is slowly becoming the standard of care for endodontics for many reasons. In a tooth with a somewhat unusual root shape, such as the case demonstrated here, CBCT helps us determine the number of canals so that we can keep our accesses minimal and make informed decisions of where to look for accessory canals such as an MB2. This tooth had a conical root shape so a CBCT was taken to determine anatomy. As you can see below, this is a highly unusual anatomy where the DB root bifurcates to form four […]
Broken Instruments...or Modified Root Filling?
BROKEN INSTRUMENTS…OR MODIFIED ROOT FILLING?
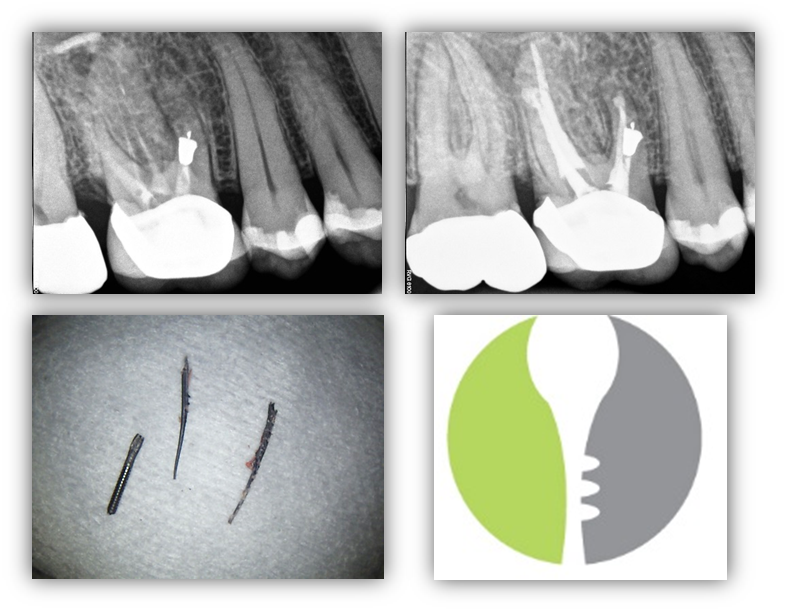
BROKEN INSTRUMENTS…OR MODIFIED ROOT FILLING? Here we present a relatively interesting case, #14, with a recurrent infection associated with the MB root. Other than pain associated with this tooth, medical history remains unremarkable. We were able to remove the “root filling” which appears to be endodontic instruments that may have also been used in initial instrumentation. In any case, we were able to remove the all three instruments and locate a previously untreated MB2 canal. This would prove to be significant as this it the only canal in the MB root that was able to be instrumented to full root […]
Read More… from BROKEN INSTRUMENTS…OR MODIFIED ROOT FILLING?
ENDODONTIC COMPLICATIONS
ENDODONTIC COMPLICATIONS
UNUSUAL RETREATMENT -
UNUSUAL RETREATMENT –

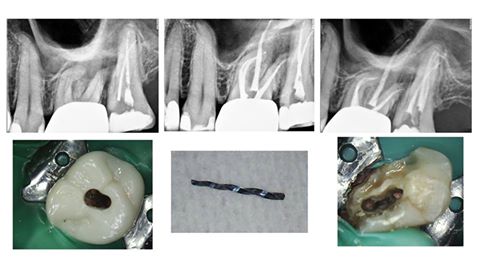
Compare the Pre Op and Post Op CBCTs to notice something unusual in this failing MB root… MB1, MB2, MB3! […]
ATYPICAL ANATOMY
ATYPICAL ANATOMY

This case represents a rare anatomic variant of a tooth anatomy much more commonly seen in the mandible: “c-shape”. Because the maxillary variant often has fused roots with DB/P canals that join very early in the pulp chamber with a separate MB canal that joins near the apex, some refer to this rare tooth as having a “semi-colon” anatomy. Take a look at the clinical photograph; can you see the semi-colon? […]