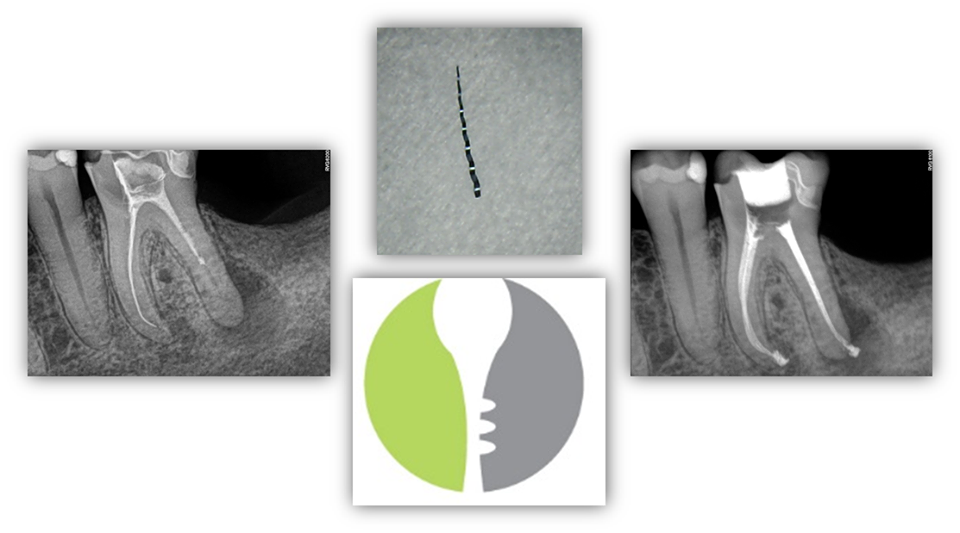
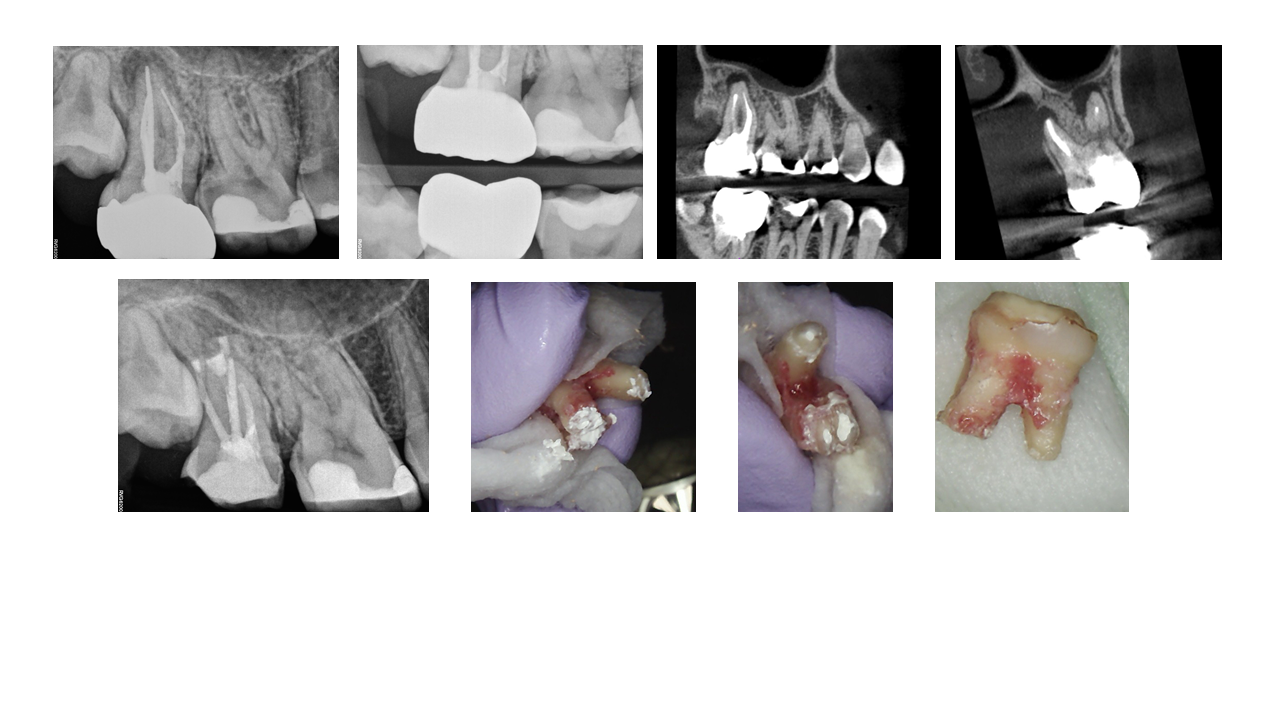
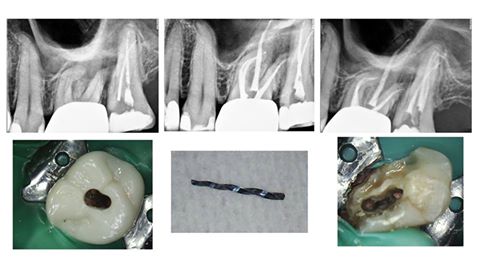
INSTRUMENT REMOVAL – This patient presented to our office with a previously initiated RCT #19 with a separated retained instrument in the ML canal. Information regarding “pathophysiology” of instrument separation, risk-benefit ratio of removing the retained instrument, alternative options if instrument removal cannot be achieved (i.e. bypass and/or apicoectomy), and prognosis were reviewed with the patient. The patient was motivated to save his tooth at all costs. Upon access, the retained instrument was visualized in the ML canal. The instrument was successfully removed using ultrasonics and hedstrom files. The patient was pleased with the final result. […]
INSTRUMENT REMOVAL