FIXING COMPROMISED CASES: This 50 y.o. healthy male presents with pain associated with the support tooth of his bridge. We have noted a 6 unit FPD with #5 and #6 used as pier abutments. We have diagnosed a recurrent infection associated with #6 secondary to a misplaced post causing a perforation on the disto-palatal aspect. As all potential options involving removal of the FPD would be very costly to replace, we made the decision to perform surgical repair of the perforated post. Root end preparation and retrofill was also done to seal off all potential communications from the canal system […]
FIXING COMPROMISED CASES
INSTRUMENT REMOVAL
INSTRUMENT REMOVAL
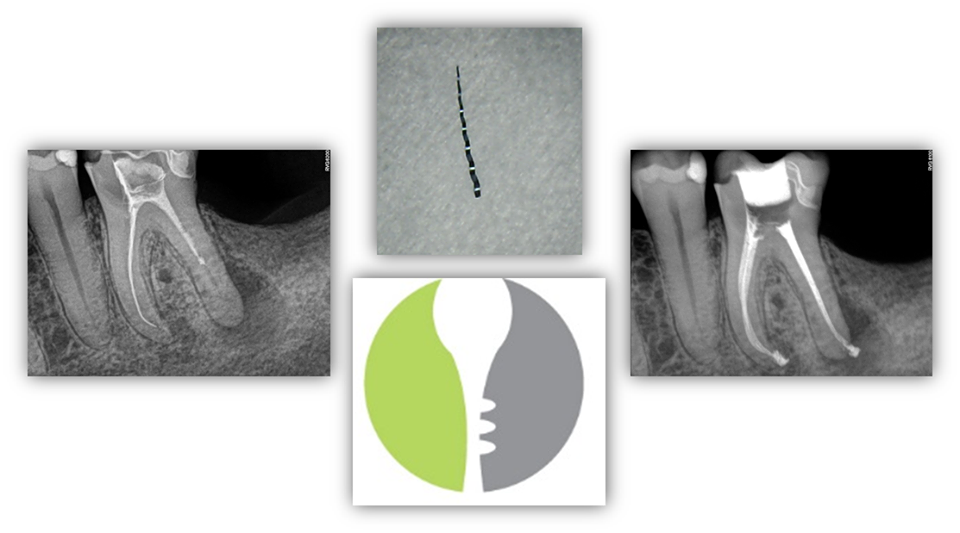
INSTRUMENT REMOVAL – This patient presented to our office with a previously initiated RCT #19 with a separated retained instrument in the ML canal. Information regarding “pathophysiology” of instrument separation, risk-benefit ratio of removing the retained instrument, alternative options if instrument removal cannot be achieved (i.e. bypass and/or apicoectomy), and prognosis were reviewed with the patient. The patient was motivated to save his tooth at all costs. Upon access, the retained instrument was visualized in the ML canal. The instrument was successfully removed using ultrasonics and hedstrom files. The patient was pleased with the final result. […]
TRANSIENT APICAL BREAKDOWN
TRANSIENT APICAL BREAKDOWN
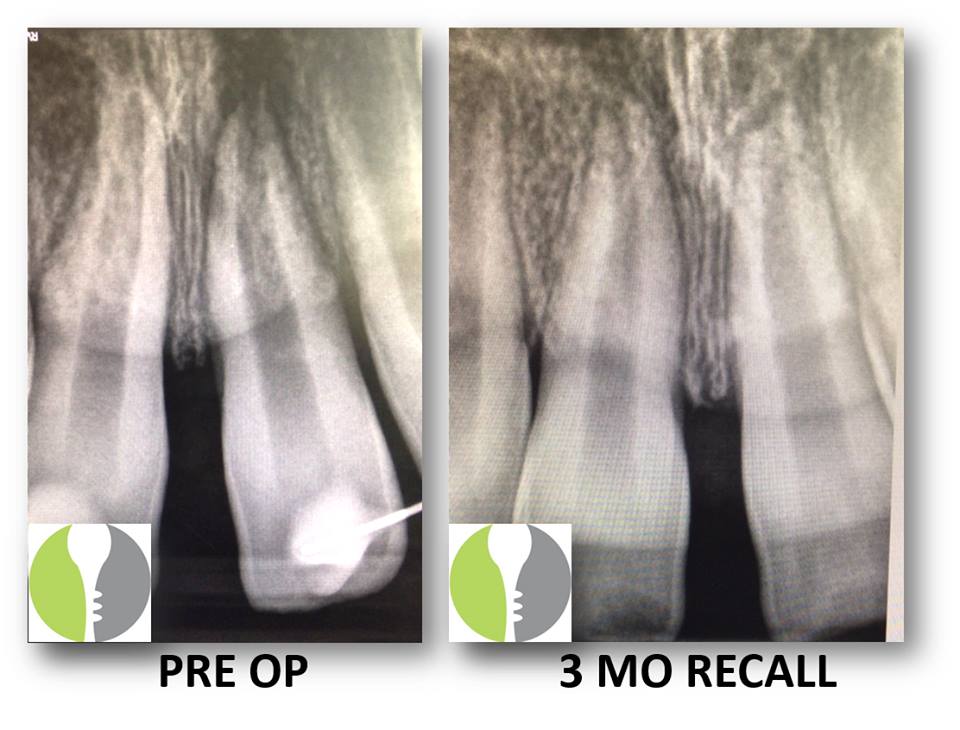
TRANSIENT APICAL BREAKDOWN: Here we present a case of a young healthy male who sustained facial trauma involving monkey bars and affecting tooth #9. He had subsequently had a splint placed at the ER to rectify a subluxation injury and was referred to our office for follow-up and necessary treatment. Upon initial evaluation, the tooth was still slightl symptomatic and tested negatively to pulp vitality testing. Additionally, there appeared to be a lesion on radiograph. As the traumatic incident was recent, we recommended that the tooth be re-evaluated at a future date (in this case 3 months) and instructed the […]
COMPROMISED CASES
COMPROMISED CASES
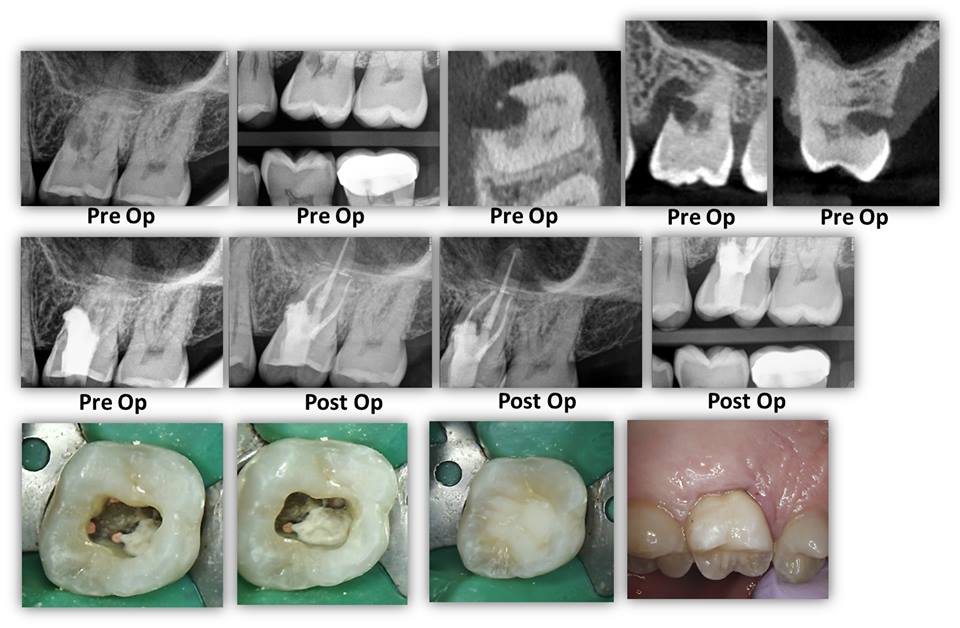
COMPROMISED CASES: Here we present a case where both restorative dentist and periodontist were a little unsure as to what could be done here with regards to the large resorption defect on the mesio-palatal aspect. Periodontal surgery was initially in the plan should the tooth be deemed restorable. We deconstructed the case via complete canal instrumentation, degranulation of the resorption defect, and medication with Ca[OH]2. On the second visit, we completed the root canal and repaired the defect with Brasseler Root Repair Material and sealed it with a dual cured core composite. At 8 weeks between treatment initiation and completion, the […]
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
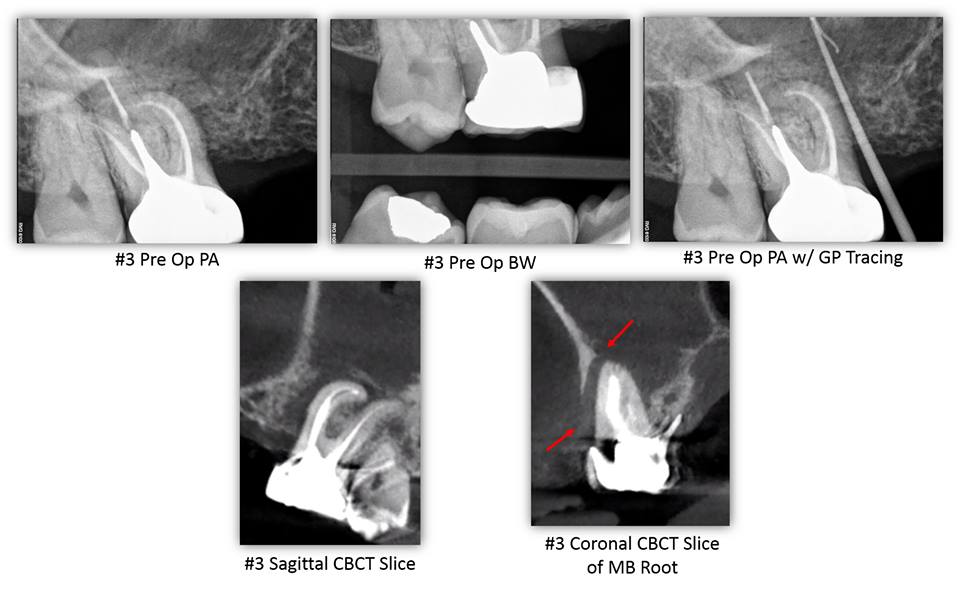
OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY– This patient presented for evaluation of tooth #3. His chief complaint was a painful swelling of gum that would sometimes bleed in the area of tooth #3. The patient reported RCT #3 was completed over 20 years ago by an Endodontist. The patient stated that he is congenitally missing teeth #4, 5, 12, and 13. The patient denies wearing an RPD. The patient’s chief complaint was consistent with a sinus tract located mesial to tooth #3 at the level of the alveolar crest. The sinus tract was traced with gutta-percha. Tooth #3 had an intact […]
Read More… from OROANTRAL COMMUNICATION CAUSED BY ODONTOGENIC PATHOLOGY
IT'S SHARK WEEK Y'ALL!!!
IT’S SHARK WEEK Y’ALL!!!

IT’S SHARK WEEK Y’ALL!!! As it pertains to the dental arena, we wish we had a bit of those shark genes…because every time we have a bad tooth, we would just pull it and grow a new one indefinitely! Unfortunately for us, but fortunately for our profession as dentists, humans don’t have that luxury. So it’s important to SAVE YOUR TEETH!!! SEE YOUR ENDODONTIST!! It’s the only set you’ll have…. […]
LAST CASE OF THE WEEK
LAST CASE OF THE WEEK

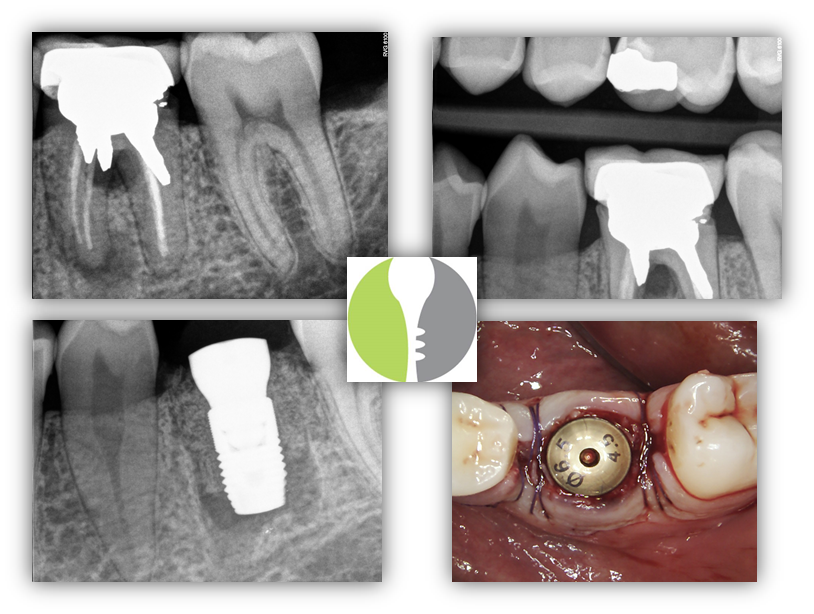
LAST CASE OF THE WEEK: Non-restorable #31 – Bridge sectioned between #29 and pontic #30 – #31 and residual root tip #30 extracted – Extraction site #31 grafted – Site #30 ridge augmented in preparation for dental implants to replace the existing FPD. […]
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT
CRACK EXTENSION DETERMINED BY CBCT – Typically, a crack cannot be identified on a CBCT scan unless the crack is large. In this case a patient presented with a large MOD crack of tooth #15. The crack was large enough that an explorer could be inserted and the buccal and palatal segments agitated. CBCT was exposed and the MOD crack can be visualized to its terminus on the palatal aspect of the MB root. Here, CBCT was a great tool for diagnosis, prognosis, and patient education. […]
Another One Bites the Dust
ANOTHER ONE BITES THE DUST
ANOTHER ONE BITES THE DUST: I was actually thinking for moment to try and save this one…but the cost:benefit analysis for retreatment, perforation repair, new indirect restoration just didn’t seem worth it. Additionally with that much retention needed in the form of the post/core), there is surely a significant compromise in the lack of good tooth structure left to work with. We decided to go with the more predictable route here. […]
Thermafill retreatment #30 with some accessory portals
Thermafill retreatment #30 with some accessory portals

Thermafill retreatment #30 with some accessory portals. Root canal completion #31. More anatomy….. […]
Read More… from Thermafill retreatment #30 with some accessory portals