[…]
Read More… from Sedation Dentistry: How It Works and What to Expect

TREATMENT PLANNING DILEMMAS: Here we present a case with an initial presentation of a history of both non-surgical and surgical treatment (of the MB root). The patient’s chief complain included persistent pain. CBCT (not shown here) confirmed a lesion associated with the MB root. Interestingly, we also noted that surgery had been done on the MB canal but not he MB2 canal due to an incomplete root resection. The apical plug associated with the MB canal was intact. With the help of the patient’s lack of motivation to pursue surgery again, the decision was made to non-surgically retreat the case. One […]
DON’T KNOW IF YOU need a root canal? These signs may just tell you. If you have any of them, don’t dismiss them and come see us as soon as possible! https://live-renovo.pantheonsite.io/ […]
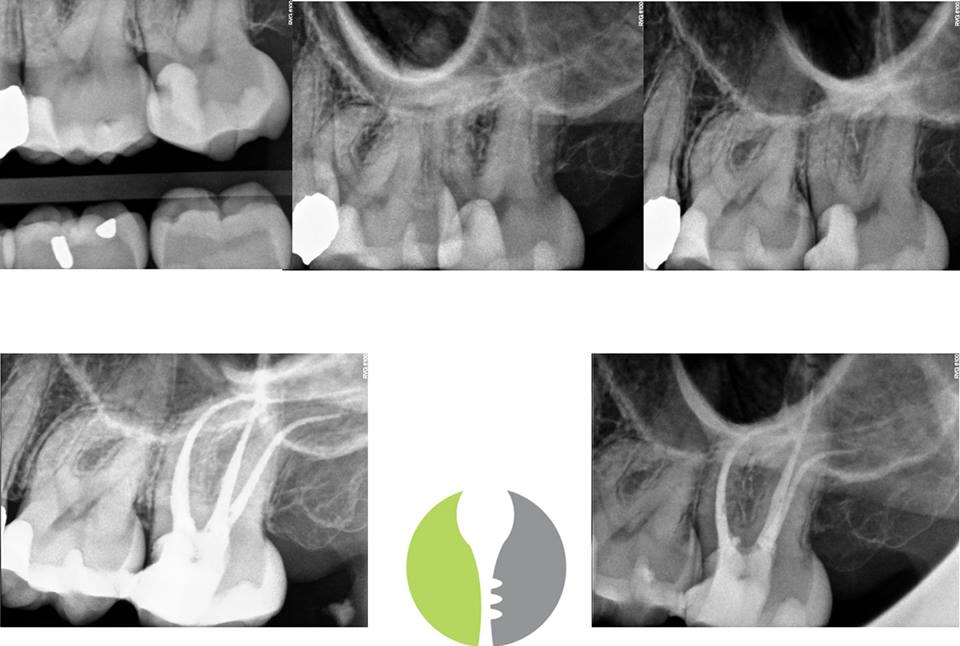
PATIENT MANAGEMENT AND ENDODONTIC TREATMENT: It is not always the anatomy that is difficult in the aspect of treatment. However, added factors can compound case difficulty such as minimal opening, unfavorable angulation towards the cheek, the position of being last tooth in the mouth, AND LONG (WL – 24mm) Curvy Calcified (MB2) Anatomy. At first glance, this just looks like a “run of the mill” root canal with some nice curvatures. However, it is important to note that we treat people, not just teeth. […]
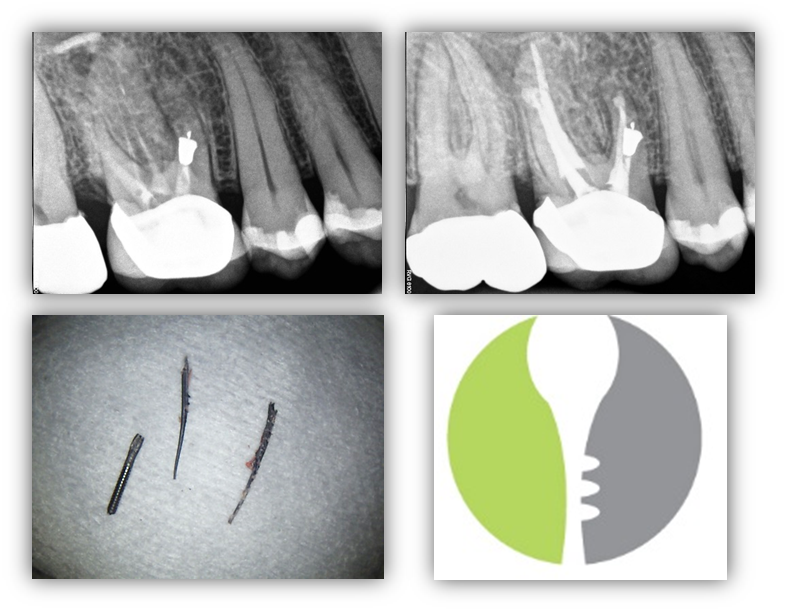
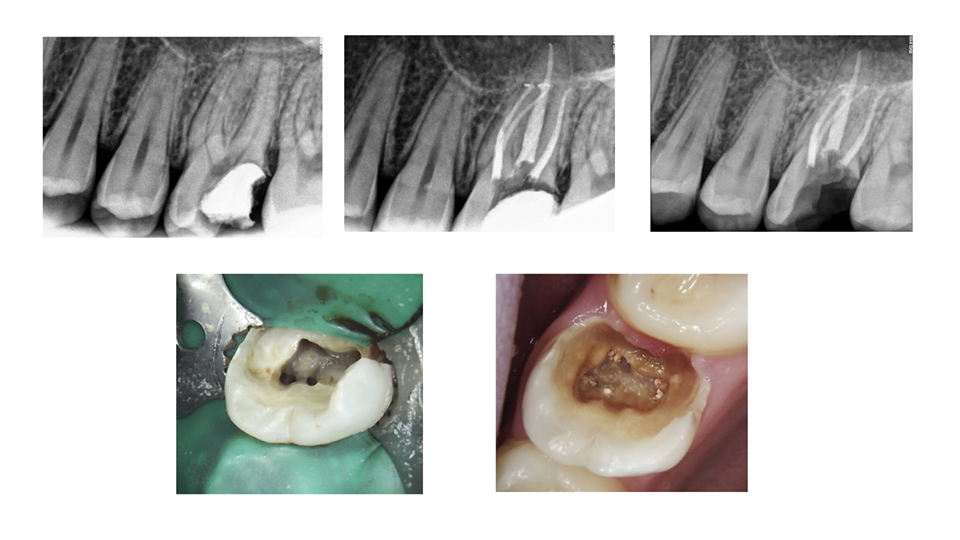
BROKEN INSTRUMENTS…OR MODIFIED ROOT FILLING? Here we present a relatively interesting case, #14, with a recurrent infection associated with the MB root. Other than pain associated with this tooth, medical history remains unremarkable. We were able to remove the “root filling” which appears to be endodontic instruments that may have also been used in initial instrumentation. In any case, we were able to remove the all three instruments and locate a previously untreated MB2 canal. This would prove to be significant as this it the only canal in the MB root that was able to be instrumented to full root […]
Read More… from BROKEN INSTRUMENTS…OR MODIFIED ROOT FILLING?
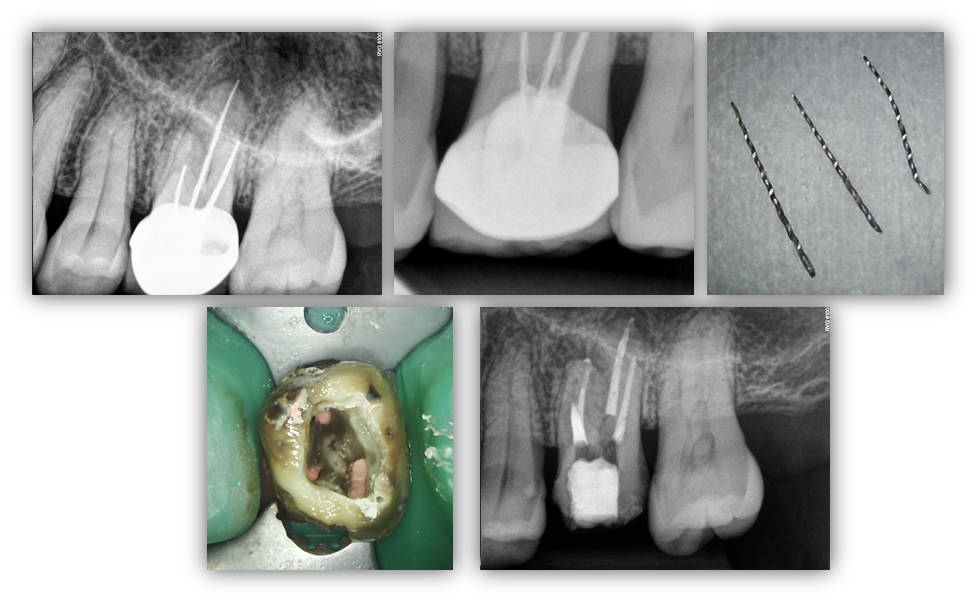
WHY IT IS USEFUL IF YOUR ENDODONTIST CAN DO PERMANENT RESTORATIVE TX: While as endodontists, we always defer core and crown fabrication to the restorative expert (the patients general dentist), we do offer core placement and crown repair for those dentists who request it of us. Here is a great example of why it can be useful to have the core build-up completed at the time of RCT. You will see intra-op photo (5 canal #14) compared with a 6 month recall with gross caries throughout the entire access after the patient failed to have the tooth restored in a […]
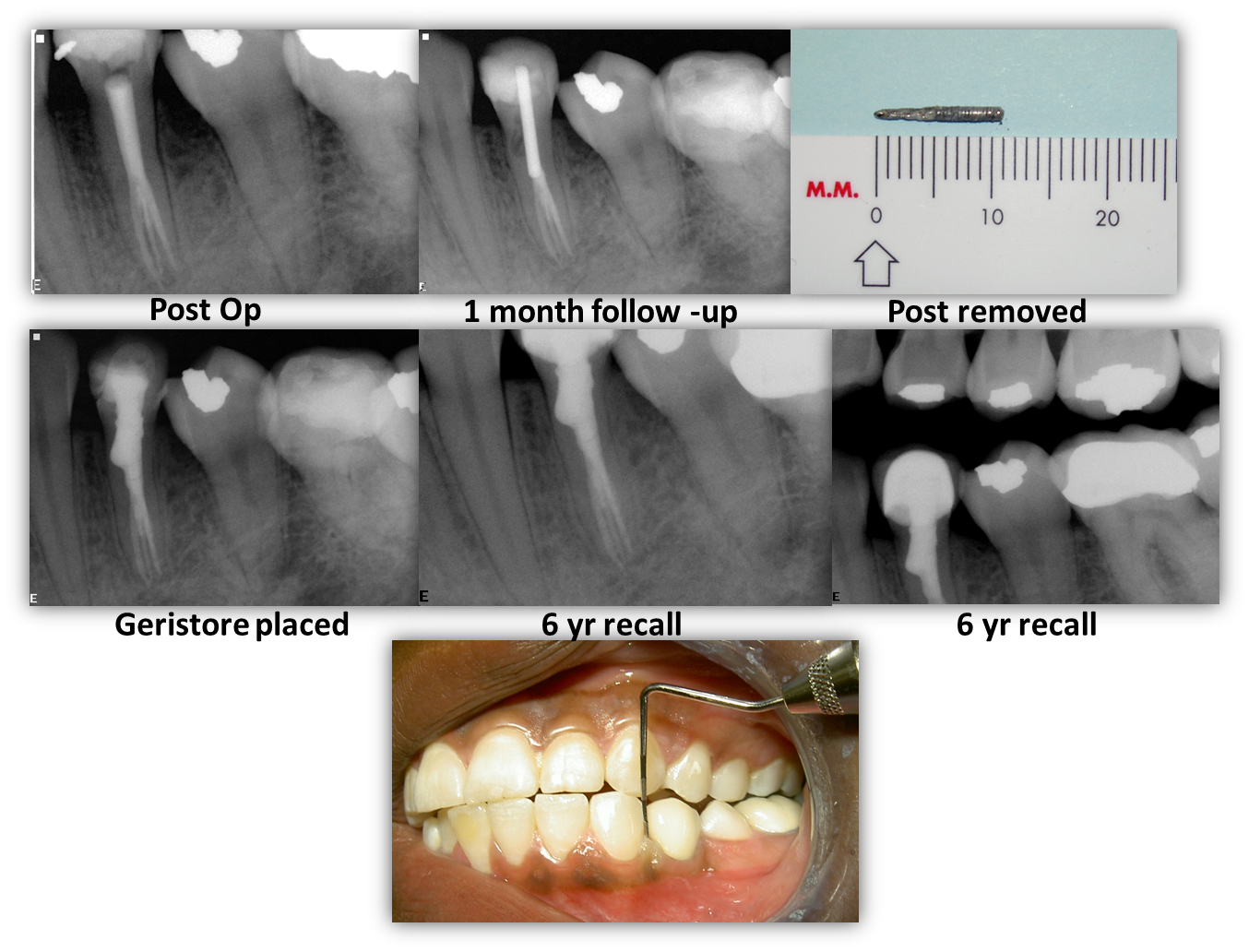
Here we present a healthy 18yo African American female in which non-surgical root canal treatment was rendered on #21 demonstrating a nice trifurcation anatomy. Some time later were we were contacted by the restorative dentist wanting us to re-evaluated the post/core placement prior to crown fabrication. As one can see, it appears that that something went awry while preparing the post space and large void had been left on the mesial aspect at mid-root level. We felt that this would compromise long term fractural resistance. Therefore, the post was removed and dual-cured core composite was placed to aid with fracture […]
Read More… from RESTORATIVE COMPLICATIONS WITH ENDODONTIC TREATMENT
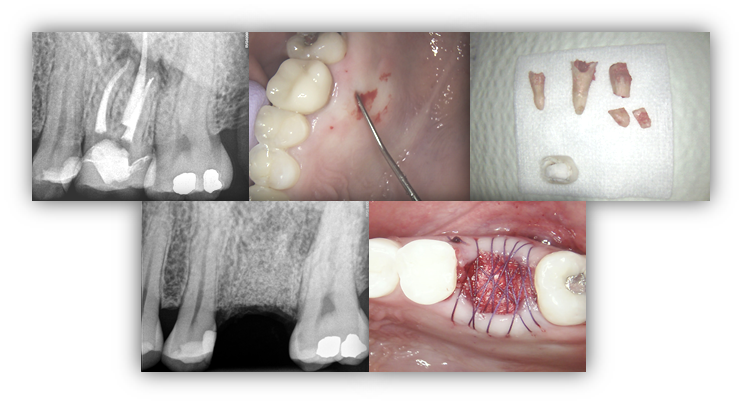
WHY IS IT BENEFICIAL FOR ENDODONTISTS TO BE PROFICIENT IN EXTRACTIONS AND SOCKET PRESERVATION? This patient presented to our office complaining of a draining sinus tract on the palatal gingiva of tooth #14. Clinically, tooth #14 had an isolated deep probing depth of 13mm on the palatal aspect with corresponding complete bone loss around the palatal root on the CBCT (not pictured below). The patient was advised that these findings are consistent with vertical root fracture and prognosis is hopeless. The patient was highly motivated to extract tooth #14 and restore with an implant. Although it is not a requirement […]

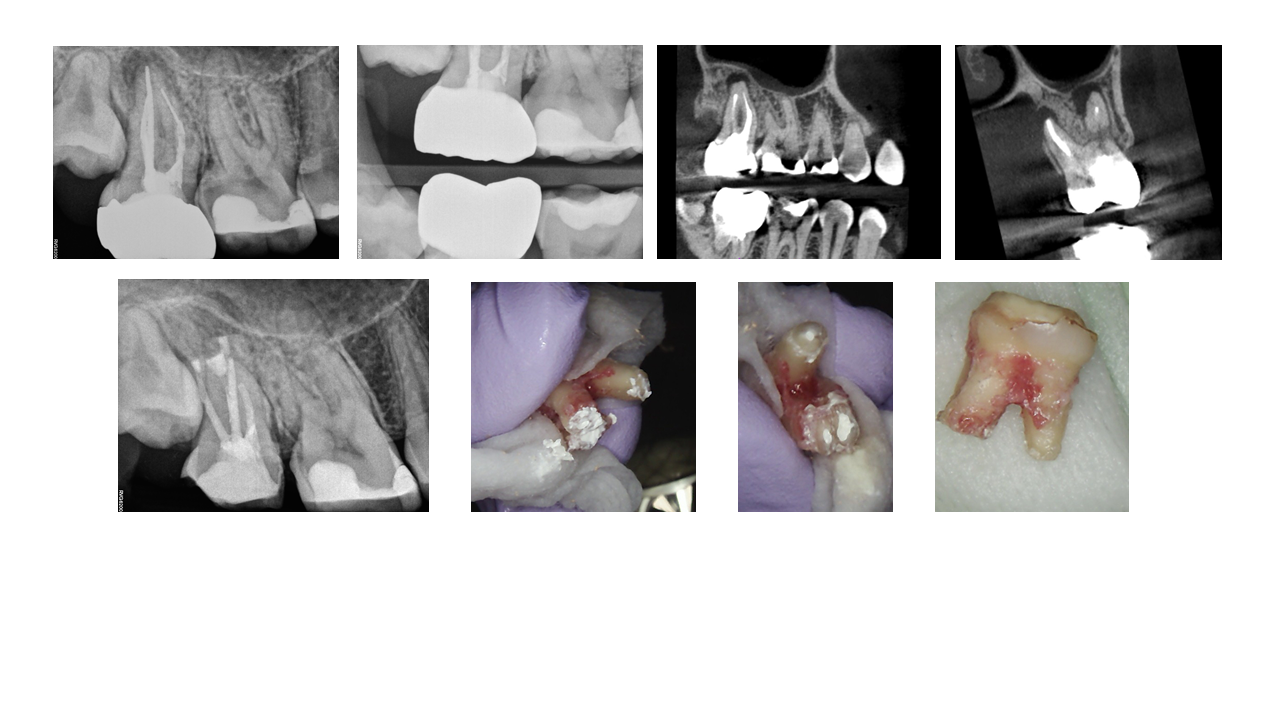
ENDODONTIC TREATMENT PLANNING DILEMMAS: Here we present an interesting case of a 47yo healthy Asian male with an exceptionally esthetic FPD #3-5 with #4 as the pier abutment. The FPD was done a little over a year prior to initial presentation to our office. The patient had subsequently presented to our office with persistent bite discomfort and pain upon digital palation of the “gums”. Although both #4 and #5 were infected, #4 had a vertical root fracture traveling from the apical –> coronal (confirmed via CBCT and subsequent surgical access). Apical surgery was initially planned on #5 and full root […]
WHY DOES MY ENDODONTIST DO EXTRACTIONS? There are several clear benefits of working with endodontists who are comfortable with extractions: (1) If a tooth is found to be non-restorable during treatment due to a severe crack or fracture, we can immediately remove the tooth while they are already numb without having to send the patient to another dentist who may not be able to see them for severaldays (2) It allows us to be somewhat ‘unbiased’ with regards to recommending either RCT or EXT treatment options. However, comfort with extractions also allows us to increase our surgical repertoire to provide […]